Saliva & Oral Health


Stimulated saliva neutralizes plaque, promotes remineralization through the increased release of calcium and phosphate ions, and assists in lubricating tissues in the oral cavity.
Saliva is certainly one of the most important components in the oral environment and an integral component to oral health. Besides lubricating the tissues, it maintains a neutral pH environment that promotes tooth remineralization from the wealth of ionic minerals available in solution, and affords antimicrobial function through immunoglobulins and proteins present in the fluid. Because most of our procedures focus on teaching patients to prevent oral disease, we need to ensure the maximum benefits that may be gleaned from a normal or enhanced salivary flow.
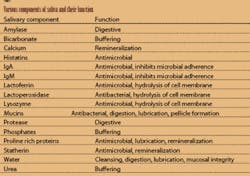
Saliva assists in digesting, diluting, and clearing dietary carbohydrates as well as buffering acid after a sugar exposure. Calcium and phosphates are maintained in supersaturation for bioavailability to remineralize the tooth structure. In addition, saliva aids in maintaining mucosal integrity and in digestion through salivary enzymes. Saliva is essential in formation of the pellicle, which protects the tooth after eruption. (See Table 1.)
Saliva is generated by three pairs of major glands (the parotid, submandibular, and sublingual) and numerous minor salivary glands, located in the lips, buccal mucosa, dorsum of the tongue, and soft palate. The major salivary glands produce 93 percent of all saliva. Water comprises 99 percent of saliva. The remaining components are macromolecules, as listed in Table 1. The viscosity of saliva depends on the components present.
Daily saliva output is in the range of 150 to 500 mL, although the average daily volume of saliva in the oral cavity is only 1mL. Mean resting saliva output is 0.4 mL/min and is highest in the morning. Stimulated saliva output, which is driven by masticatory or gustatory signals, is between 1 to 2mL/min. When the saliva is stimulated, there is an increase in the bicarbonate ions, which causes a rise in the pH, increasing the buffering power against a carbohydrate event.
Saliva has several oral benefits including buffering, remineralization, and lubrication. Consider the acid attack on the teeth after a cariogenic episode. For 20 to 30 minutes after ingesting a sugar product, there is a drop in pH due to acid production by the oral bacteria. Interestingly, after this sugar episode, the production of saliva ceases once swallowing occurs. The saliva output returns to a resting state within a short time. The tooth is most susceptible during this time period.
The old adage that we miss something when it is gone rings true with saliva. We truly see saliva’s myriad of benefits once its flow is slowed or stopped. Since saliva aids in mechanically removing food debris and bacteria from the oral cavity and teeth, reduced salivary flow causes ill effects to the oral tissues. Xerostomia has several etiologies, including simple mouth breathing, drug manifestations, hormonal fluctuations, autoimmune diseases, neurological or psychogenic disorders, and aging. Patients may also exhibit a decreased function of the salivary glands through neoplasm, trauma, surgical intervention, or sequellae of radiation therapy. The main consequence of xerostomia is a dry, burning mouth, which will affect a patient’s ability to swallow, taste, speak, and maintain oral tissue integrity. Demineralization of enamel, an increased caries rate with rapid progression of the lesions, and an overgrowth of Candida will also occur.
Stimulating saliva with chewing gum
Saliva must be present in the oral cavity to preserve the integrity of both hard and soft tissues, therefore it is imperative to maintain normal salivary flow during the day. Stimulation of saliva by nonfood products such as sugarless chewing gum offers an increased flow rate with no detrimental effects on the oral structures.
Although the average American chews about 300 sticks of gum a year, gum has been given a bad rap by some clinicians. In 1869, a physician wrote that chewing gum would “exhaust the salivary glands and cause the intestines to stick together.” With modern medicine came the knowledge that gum does not cause those maladies, nor does it lead to clicking and popping of the TMJ. Current research has indicated many positive oral benefits from chewing gum, mainly focusing on the stimulation of saliva, remineralization of enamel, and control of oral pH.
A quick history of gum is rather fascinating. Initially, chewing gums were made from tree resins. Mastiche, a resin from the mastic tree, was first used as gum by Greeks in 50 AD. The term “masticate” is generated from this Greek derivative. South American Mayans utilized chicle while North American Indians utilized spruce resin. Paraffin and other waxes were also chewed, but were not as popular as the resins. The first commercial gum, made by Curtis Brothers, didn’t appear until 1848. Although these first chewing gums were made from spruce, paraffin was later added for a more chewable product. Dr. William L. Semple, a dentist, patented the first chewing gum in 1869. In 1871, the first licorice-flavored gum was introduced and sold like wildfire. Sugar was not added to gum until the 1880s by the Fleer Company, which also made the first bubble gum. Sugarless gum, which now seems very retro as the original products contained only resins, was introduced in the 1950s by Dr. Petrulis, a Naperville, Illinois dentist.
Chewing paraffin or gum increases salivary flow. With mere chewing stimulation, the salivary glands produce more fluid. With the increased salivary flow, there are more ions, such as bicarbonate, to neutralize acids, in addition to calcium and phosphorous available to remineralize dental enamel and buffer the pH. When there is a combination of taste or flavor added to the mastication component, there is a 10-fold increase in flow rate. Stimulated flow of saliva continues for 20 minutes after chewing.
Chewing sugarless gum containing either sorbitol or xylitol increases salivary flow. This stimulated saliva enhances the release of more bicarbonate ions, facilitating buffering capacity and raising the pH after a sugar incident. The 20- to 30-minute acid attack on the teeth after the sugar ingestion will be counteracted by the increased volume of saliva and rise in pH. Increasing the bicarbonate ions decreases the potential harm of organic acids on enamel hydroxyapatite crystals. Additionally, the increase in salivary fluid volume assists in oral clearance, hence removing more of the intraoral acid created from the carbohydrate incident.
Chewing gum for 20 minutes after a sugar exposure also promotes remineralization by raising the amount of available calcium and phosphate ions in the salivary fluid. The stimulated salivary flow enables more salivary ions to be available in solution for remineralization of the tooth, allowing for the protective capability of saliva.
The mechanical cleansing of the teeth adds to the anticaries effect of the sugarless gum. Food is cleared from the oral cavity, and plaque is removed from the occlusal surfaces. Although smooth surface plaque remained unaffected, up to 44 percent reduction in the plaque on the occlusal surface was found. This follows with the evidence that normal oral movements of swallowing and chewing will cleanse the buccal, occlusal, and lingual surfaces of the teeth, but the gingival margin will be unaffected, hence the need for proper brushing techniques in the sulcular area. As the occlusal table is the most susceptible to caries, oral debris clearance and plaque removal from this site is beneficial.
Measuring saliva in the near future
Sugarless gum is also used as a vehicle to deliver medicaments that may benefit oral and systemic health. Sugar and sugar substitutes are not the only additives in gum products. Products for caries reduction, which increase enamel resistance or neutralize plaque acid, and components for tooth whitening and breath freshening are formulated into chewing gum. Sodium fluoride, chlorhexadine, carbamide, bicarbonate, calcium phosphate, and zinc component chewing gums are on the market both in the United States and overseas. Delivery of systemic medicaments, such as methadone, acetylsalicylic acid, miconazole, and vitamin C are also available. Nicotine cessation gums are currently components of anti-smoking therapy. All increase salivary stimulation while releasing specific active substances directly into the oral cavity. Other medications, such as Viagra, are currently being evaluated for future delivery via chewing gum.
How do we determine if there is an adequate amount of saliva present? Products are available on the market to monitor salivary flow. Saliva Check (GC America) offers a testing system that assesses resting salivary pH, salivary consistency, stimulated salivary flow, stimulated salivary pH, and buffering capacity. Single-dose kits prevent cross contamination and contain a collection cup, unflavored paraffin, saliva pH test strips, and buffer test strips. Results are known within two minutes. It is an effective tool to evaluate quality and quantity of saliva, identify saliva problems, and assist in treatment planning. As a tool to identify salivary dysfunction to the patient, it will facilitate discussion of the possible etiologies of xerostomia and preventive management modalities.
Stimulated saliva neutralizes plaque, promotes remineralization through the increased release of calcium and phosphate ions, and assists in lubricating tissues in the oral cavity. Sugarless gum assists in delivering all of these great oral health benefits. Knowing the popularity of gum, we have the ability to capitalize on the positive reinforcement of suggesting chewing gum as an adjunct to oral care, especially when the proper oral physiotherapeutic devices are unavailable or inaccessible. What an incredibly painless addition to our preventive recommendations for our patients.
Sheri B. Doniger, DDS, has been in the private practice of family and preventive dentistry for more than 20 years. A dental hygiene graduate of Loyola University prior to receiving her dental degree, her current passion is focusing on women’s health and well-being issues. She may be contacted at (847) 677-1101 or [email protected].
References
Doniger, SB, “Saliva, Chewing Gum and Dental Health” Dentistry Today, September 2004 Vol. 23 No. 9, 136, 138, 140-1.
Saliva Check Product Information .pdf, “Saliva - Natural Caries Defense Patient Check up Kit” GC America, Alsip, Ill.