OUCH! DENTINAL HYPERSENSITIVITY REVISITED


Dentinal hypersensitivity is short, sharp pain from exposed dentin in response to stimuli. These are usually mechanical, evaporative, thermal, tactile, osmotic, or chemical, and cannot be attributed to any other form of dental pathology or defect. Patients often turn to hygienists for advice. But the sad fact is that while many patients have dentinal hypersensitivity, the majority never reports it or seeks relief. Sometimes their excuse is “I don’t want to bother the dentist.”
Dentinal hypersensitivity has been extensively researched. Many in the field agree the condition is either underreported or misdiagnosed.
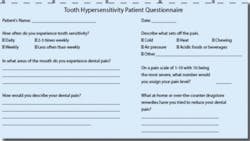
Questions the hygienist may ask a new patient are, “Are you experiencing any problem areas or are you concerned about anything in your mouth today?” Or, “Have you noticed any sensitivity of your teeth or gums recently?” This opens the door to dialog with the patient. A questionnaire included in this article can be duplicated for use at chairside.
The prevalence of cervical dentin hypersensitivity is estimated to range anywhere from 45 percent to 57 percent of the adult population. Nearly 30 percent of all adults experience dental hypersensitivity at some time in their lives. The occurrence is significantly higher in patients who undergo periodontal treatment - 60 percent to 98 percent. This stems from recession following surgery or from loss of cementum following nonsurgical periodontal therapy.
Theories behind dentinal sensitivity
The most widely accepted explanation of the cause of dentinal hypersensitivity is the hydrodynamic theory. This occurs when various stimuli cause rapid outward flow of fluid contained in the dentinal tubules. This rapid release of fluid creates a pressure change across the dentin that stimulates nerve fibers and results in pain. Cold is the most common stimulus of dentinal hypersensitivity. Other common causes include periodontal disease and improper brushing habits that result in gingival recession.
Hypersensitivity is most commonly reported on the facial surfaces of the canines and first premolars, followed by the second premolars and incisors.
Patients can often assist in the diagnosis by identifying the pain-inducing stimuli, such as thermal, tactile, etc., as well as describing the pain. One patient held her hand to her face and said, “The pain comes like a bolt of lightning! Ice cream and iced tea can trigger an instantaneous jolt of pain!”
Sometimes the most fastidious of patients experience hypersensitivity due to gingival laceration from overly exuberant toothpicking or toothbrush abrasion. “I thought I was doing a good thing,” one enthusiastic patient commented.
One of the most common reasons for exposed dentinal tubules associated with hypersensitivity is a predisposing factor - gingival recession. Bacterial plaque, inadequate gingiva attached, crown preparation, and gingival loss secondary to disease or periodontal surgery can all cause gingival recession. Areas of recessed gingiva may be sensitive due to the loss of cementum, which ultimately exposes the dentin.
Treatments for dentinal hypersensitivity - noninvasive and invasive
Treatment success depends on the underlying cause and extent of the pain, as well as the patient’s willingness to change behaviors. If the dentinal hypersensitivity is due mostly to patient behavior(s), it may be difficult for patients to change. If the diagnosis confirms dental hypersensitivity in the absence of underlying diseases or structural problems, the hygienist can initiate the following steps to gain patient cooperation:
• Remove the apparent risk factors by educating the patient about dietary acids and modifying the oral home-care regimen
• Recommend modified tooth-brushing methods as determined by the patient’s willingness to cooperate
• Recommend a desensitizing regimen for home use, such as fluoride gels and/or mouth rinses and antihypersensitivity toothpastes
• Apply topical desensitizing agents in the office such as gels, varnishes, iontophoresis, primers containing HEMA, glass ionomer cements, and adhesive resins
The hygienist should initially recommend noninvasive treatment methods such as topical agents and dentifrices that contain a desensitizing active ingredient. Potassium nitrate is the most common desensitizing ingredient in toothpaste. The potassium ions block the synapse between nerve cells, reducing nerve excitation and its associated pain. Another active ingredient with similar action is potassium chloride.
Reducing the flow of moisture into the dentinal tubules by occluding or sclerosing the tubules is another noninvasive treatment. Active ingredients that effectively accomplish this include stannous fluoride, strontium chloride hexahydrate and aluminum, and potassium or ferric oxalates.
Other ingredients that are effective desensitizing agents include dentin sealers (resins), sodium monofluorophosphate, and sodium citrate.
If non-invasive treatment doesn’t work, invasive treatment options performed by the dentist may be required. These include gingival surgery, application of resins, or a pulpectomy.
Some offices have found dental lasers to be effective in the treatment of dental hypersensitivity. Theories are that the mechanism of action is the coagulation and precipitation of plasma proteins in dentinal fluid, or the possibility that the thermal energy alters intradental nerve activity. Another consideration is the substantial investment of lasers.
Sensitivity associated with dental procedures
Tooth sensitivity is a significant side effect associated with tooth-whitening procedures. The incidence of hypersensitivity associated with tooth bleaching reported in clinical trials ranged from less than 10 percent to greater than 50 percent. One recent clinical trial and literature review concluded that mild sensitivity could be expected in 50 percent of patients, moderate sensitivity in 10 percent of patients, and severe sensitivity in less than 5 percent of patients. In many instances, the sensitivity associated with bleaching is transient and resolves on its own.
Contributing factors to sensitivity associated with tooth bleaching include too frequent changes of the bleaching gel; gingival recession; and pressure from the tray (stent).
A higher incidence of sensitivity has been associated with longer application times and higher concentrations of bleaching solution. Therefore, it makes sense for patients to administer the solution over a shorter application time when using higher concentration products.
Many of the at-home administered bleaching gels contain glycerin, a desiccant associated with tooth sensitivity. At least one manufacturer has substituted propylene glycol for glycerin. Several at-home products now contain fluoride and potassium nitrate, which seems to reduce sensitivity. Clinical trials have shown that carbamide peroxide gels containing these additives cause significantly less tooth sensitivity than other gels.
When sensitivity is associated with at-home whitening, the patient should reduce the time and frequency of application. In severe cases, the patient may need to discontinue bleaching until the sensitivity is resolved. Using gels that contain 5 percent potassium nitrate and 1,000 ppm fluoride ion can also help reduce the sensitivity associated with tooth bleaching. These can be applied with a customized bleaching tray. Another technique is the application of potassium nitrate desensitizing dentifrices directly into the custom tray. This is a desirable option because it is less expensive, can be purchased over-the-counter, and can be used by the patient whenever necessary.
Another cause of hypersensitivity is direct restorations. Most sensitivity is minor, and is usually resolved within 30 days following treatment, especially in Class I posterior composite restorations.
The type of adhesive and how it is used may also have a correlation to postoperative sensitivity in posterior composites. Of the offices surveyed, many reported less tooth sensitivity with self-etch systems. When the smear layer is completely removed during etching, the dentinal tubules become exposed and enlarged. Resin adhesive must seal this surface well to reduce the potential for sensitivity. The difference is the self-etch systems tend to modify rather than remove the smear layer, and resin impregnation occurs simultaneously with conditioning. The tubules are then less likely to be opened, surface sealing is more predictable, and sensitivity is less likely.
Another simple and predictable method to reduce postoperative sensitivity is to apply resin-modified glass-ionomer liner.
Hygienists need to be aware of the causes and treatments for dental hypersensitivity. Questioning the patient during the initial interview may highlight the patient’s concerns about hypersensitivity and may prompt him or her to seek relief. When hygienists are aware of the causes, hypersensitivity may be prevented and treatment may be more effective.
Diagnosis of Dentinal Hypersensitivity
When making a diagnosis, a thorough examination should be done to rule out other contributing factors to pain. Useful diagnostic items include:
• an air-water syringe (thermal testing)
• dental explorer (touch testing)
• bite stress tests
• percussion testing
• other thermal tests, including an ice cube and occlusal assessment.
The rationale for conducting a complete dental exam is to rule out other conditions with sensitivity, such as:
• dental caries
• a cracked or chipped tooth
• a fractured restoration
• gingival inflammation
• postrestorative sensitivity
• marginal leakage
• pulpitis
Excessive consumption of dietary acids, such as citrus juices and fruits, carbonated beverages, wines, and ciders has also been identified as potential risk factors associated with dental hypersensitivity.
During the examination, other risk factors may be evident, such as:
• toothbrush abrasion
• chemical erosion
• gingival recession
• thinning enamel
• exposed dentin
• gastric reflux or eating disorders (such as anorexia-bulimia)
Etiology of Dentinal Hypersensitivity
Tissue loss and exposure of dentinal tubules
• Tooth substance loss (enamel and cementum)
Opening of dentinal tubules/removal of smear layer
• Acid in dental plaque, diet, gastric reflux
• Agents in toothpaste such as abrasive of surfactant
• Vital bleaching
Stimulation of dentin hypersensitivity
• Temperature (cold drink, ice cream, cold water, etc.)
• Overzealous tooth brushing or flossing
• Acid in diet or gastric reflux
• Poor oral hygiene
In-office Treatments for Hypersensitive Dentin
Treatment agents that do not polymerize:
A) Varnishes/precipitants
1. Shellacs
2. 5% NaF varnish
3. 0.4% SnF2, 0.14% HF solutions
4. 3% monopotassium-monohydrogen oxalate
5. 6% acid ferric oxalate
6. Calcium phosphate preparations
7. Calcium hydroxide
B) Primers containing HEMA (hydroxyethyl methacrylate)
5% glutaraldehyde, 35% HEMA
Treatment agents that undergo setting or polymerization reactions:
1. Conventional glass ionomer cements
2. Resin-reinforced glass ionomers/compomers
3. Adhesive resin primers
4. Adhesive resin bonding systems
Use of mouth guards with gels
Iontophoresis
Lasers
References
1) Dietz E. Treatment and Diagnosis of Dental Hypersensitivity. NADA: Falls Church, VA 2006.
2) Holland GR, et al. Guidelines for the design and conduct of clinical trials on dentine hypersensitivity. J Clin Periodontal. 1997;24:808-813.
3) MacCarthy, Denise. Dentine hypersensitivity: a review of the literature. J Irish Dental Assn. Vol. 50(1), Spring 2004.
4) Pashley DH. Potential treatment modalities for dentine hypersensitivity: in-office products. In: Tooth wear and sensitivity: Clinical Advances in Restorative Dentistry, Edited - Addy, Embry, Edgar, Orchardson. 2000; London: Martin Dunnitz; 351-365.
5) Swift EJ, DMD. Causes, Prevention and Treatment of Dentin Hypersensitivity. Compendium, Vol. 25, No. 2. Feb. 2004.
6) Walters, PA. Dentinal Hypersensitivity. J Cont Dent Pr. Vol. 6, No. 2, May, 2005.