Oh my! Vampires and werewolves
by Nancy W. Burkhart, RDH, EdD
[email protected]
The modern-day craze associated with the insatiable yearning for knowledge related to vampires may be somewhat attributed to John William Polidori, the true author of "The Vampyre," published in 1819 in New Monthly Magazine. The fascination with vampires and werewolves has continued to grow with new movies such as the recent Twilight series. Multiple books such as Nancy Garden's 1973 book, "Vampires" and author Anne Rice's book "Interview with the Vampire" in 1976, as well as the "Vampire Chronicles" are probably at the root of our current preoccupation. Bela Lugosi's 1931 portrayal of Dracula has been replicated many times, and Dracula is a favorite Halloween costume with the usual fangs and blood-stained mouth against pale skin with a flowing black cape.
Various cultures present different interpretations and explanations for super humans, animal metamorphosis, witches, and supernatural behavior. Even in early Christian writings, some individuals could become transformed into various animals and inanimate objects. Vampires seem to exist independently, yet in a symbiotic relationship with the werewolf. The two creatures appeared to dominate the literature in medieval times, as well as in the documents of the early Mesopotamians and the Sumerians. Additionally, in medieval Europe, werewolves (also known as lycanthrope) were cremated in a preventive ritual so that they would not return to earth as vampires. The land most associated with vampires is Romania (specifically Transylvania). In Romania, the strigoi morti (vampires) were kept away with garlic and holy symbols. Wild roses kept them from leaving their graves. All of these techniques kept vampires away along with the usual staking, killing with silver bullets, and decapitation required for final rest. The creatures were known to remain contained as long as the sun was shining, and their thirst for blood would only surface as they searched for prey at night.
But how did one become a werewolf? In some European cities, it was stated that a person could be afflicted by sleeping outside on a summer night with a full moon shining directly on his/her face. Additionally, other methods thought to bring about the change were magic salves, wolf clothing such as a belt that is worn until one is transformed, or drinking water from enchanted streams. Contagion has been suggested, as well as rabies, in the bizarre behavior of werewolves and vampires, since folklore suggested that the person bitten became a werewolf and exhibited similar behavior. The stories state that it is passed on from one person to another, indicating contagion. This may explain the behavior if rabies were involved and why the person becomes hostile, and possibly bites or attacks another person, ultimately becoming mad.
Folklore is passed on from generation to generation and may vary according to cultural mores and geographic location. The stories and beliefs associated with werewolves and vampires originated in European countries, but similar stories with varying transformations and animal forms may be found in most cultures. The legend and stories appear to be told in almost all countries, although different names may be linked to specific geographic locations. Various cultures continue to change and add to the stories in order to meet the needs of the particular society. Fairies and leprechauns that are noted specifically in Ireland are examples of entities that take on a life form with particular personality and distinct physical characteristics.
However, the physical description of all the reported cases of werewolves and vampires appear very similar across different geographic locations. Some disease states may have actually played a part in creating the fear that fueled the frenzy in small villages where imagination along with physical characteristics of the entity became somewhat embellished and created the legends that we read about today.
One disease state that may have caused an individual to suffer such a fate is that of congenital erythropoietic porphyria. It is not unusual for such mistakes to occur. The witch trials in Salem are an excellent example. Linda Caporael, a graduate student, wrote a paper on the subject of the witches of Salem and the connection to the very strange behavior of those pronounced to be witches by the Salem residents. Ultimately, the behavior has been attributed to ergot poisoning (a fungus) through a rye crop consumed in the winter of 1691-1692. The signs of the poisoning were so similar to the hallucinations, convulsions, bizarre skin sensations, and other unusual behavior that were documented in journals. The unexplained behavior began a frenzy within the small community, resulting in the trials and burnings.
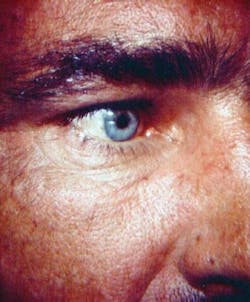
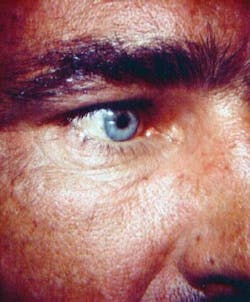
Figure 1: Note the thickened brows and orange skin color. Courtesy of Dr. Ronald Brown, Howard University.
Perhaps congenital erythropoietic porphyria may be another in a series of distinct characteristics that were not well understood by the early communities.
Types of porphyria

Figure 2: Note darkened tooth color and pebbled skin surface. Courtesy of Dr. David Wray, University of Glasgow.
- Congenital erythopoietic porphyria (CEP) (also called Gunther's disease)
- Porphyria cutanea tarda (PCT)
- ALA dehydratase-deficiency porphyria (ALADD)
- Acute intermittent porphyria (AIP)
- Hereditary coproporphyria (HCP)
- Variegate porphyria (VP)
- Erythropoietic protoporphyria (EPP)
CEP is an autosomal recessive disorder, and other forms of porphyria are classified as autosomal dominant. Porphyria may occur in seven various forms with a designation of acute, cutaneous, or both classifications. These forms include: ALADD, AIP, CEP, PCT, HCP, VP, and EPP.
Heme is the prophyrin chelate of iron – the oxygen carrying, color furnishing, prosthetic group of hemoglobin. Porphyria is characterized by excessive excretion of porphyrins or their precursors. Kooijman and Brand (2005) state that a deficiency in any one of the seven enzymes that are required results in porphyria, and the individual is unable to complete heme synthesis. The disorder results from alterations in the enzyme responsible for a step in heme production.
A heme molecule is composed of porphyrin (hence the name porphyria). An important component in hemoglobin, the molecule carries oxygen to the blood. The most common form of porphyria is porphyria cutanea tarda. Acute intermittent porphyria is a common form as well, and has been reported most often in Sweden and Great Britain.
The congenital form (CEP), also known as Gunther's disease, is characterized by the enhanced porphyrin formation of erythroid cells in bone marrow. Uroporphyrins, byproducts of porphyrin metabolism, accumulate in the skin, blood, urine, and other body tissues, producing a red/brown appearance.
Teeth and skin characteristics: A unique characteristic of CEP is the ability of the uroporphyrins to accumulate in other tissues such as the teeth, producing a red/brown color as depicted in Figure 2. When exposed to ultraviolet light, the skin and teeth will fluoresce and may appear red in color – on a bright moon-lighted night.
The skin is affected as well with vesicle-like lesions when the uroporphyrins are activated by sunlight. Photosensitivity is characteristic in a patient with porphyria, and the person will avoid sunlight only to be seen at night. They tend to be very pale from the lack of sunlight in severe cases.
Hirsutism may be extensive in patients with porphyria. Full body hair has been noted, giving the person an animal-like appearance. The skin is known to cause vesicle-like lesions with a red exudate or, in milder cases, an orange exudate. The red exudate will also appear fluorescent in moonlight or ultraviolet light. Figure 1 depicts the bushy eyebrows and the orange tint of the skin in a mild case of porphyria.
The hands may even become extremely scarred and they may take on a claw-like appearance due to deformity and excess tissue. Bright red urine is another characteristic feature. Abdominal pain, enlarged spleen, psychological symptoms, and seizures may be evident as well. In some forms, hysteria, anxiety, depression, phobias, psychosis, and delusions have been reported. In Europe and small villages, the congenital form of the disorder may be responsible for the origin of the werewolf and the legends that have ensued to this day. Illis (1964) made the case for the mysterious similarity of porphyria and tales associated with werewolves.
King George III was believed to be affected by a variegate form of porphyia caused by certain chemicals such as arsenic. The hair analysis of the king revealed high levels of arsenic, which probably affected the heme biosynthesis. It is hypothesized that he may have inherited the inborn error of metabolism that causes porphyria and was given contaminated medicines, which were common at that time, and probably promoted the disorder. It is believed that his ancestor, King James, also suffered from a condition with characteristics similar to porphyria. Even medications that are used in psychiatric illnesses today may place susceptible patients at risk for porphyria.
Oral treatment: The red/brown discoloration in teeth may be more pronounced in deciduous teeth since the disorder affects both the enamel and dentin in formation. The dentin only is affected in permanent teeth (Neville et al. 1995).
Some medications that are commonly used are contraindicated, so working closely with the patient's physician is suggested. An example would be a contraindication of lidocaine, mepivacaine, barbiturates, mercury compounds, aluminum, copper, alcohol-containing rinses, and dapsone (More, Coke 2000). Obviously, the use of sunscreens and lip balms with SPF protection, and frequent recall appointments are recommended.
The high carbohydrate diet that is considered beneficial for these patients also makes them more at-risk for caries, indicating a need for more frequent dental maintenance appointments. The condition can be exacerbated by excess alcohol, oestrogens, iron supplements, hepatitis C, and various chemicals, depending upon the type of porphyria. Higher rates of both hepatitis C and other bloodborne agents are always a consideration.
As with most rare disease states, patient education is a crucial consideration. Often, the patient may welcome the advice and any literature that can be provided to them regarding their health and oral conditions. Patients with rare disorders feel isolated and probably do not know anyone else with their condition. Support groups, close family, friends, and professionals who are informed about the disorder help add to the quality of life for the person.
The very characteristics of porphyria, may have propagated the legend of the werewolf/vampire in early years. As with the witch trials in Salem, when we do not understand the clinical manifestations of a disease state, fear is sometimes a result.
Keep asking good questions and always listen to your patients! The mind is powerful.
References
Caporael LR. Ergotism: The Satan Loosed in Salem? Science 1976; 192:April, 21-26.
Cernik C, Haller N, Mostow EN. Adult-onset Erythropoietic Porphyria in the setting of MDS. Arch Dermatol 145:8 Aug 2009.
Cox TM, Jack N, Lofthouse S, Watling J, Haines J, Warren MJ. King George lll and porphyria: an elemental hypothesis and investigation. Lancet 2005; 366:332-35.
llis, L. (Jan 1964). "On Porphyria and the Aetiology of Werewolves." Proc R Soc Med 57: 23-6.
Kessler H. (2008) Abnormalities of the Teeth (pg. 512), In DeLong L, Burkhart NW. General and Oral Pathology for the Dental Hygienist. Baltimore, Lippincott, Williams and Wilkins.
Kooijman MM, Brand HS. Oral aspects of porphyria. Int Dent J. 2005; 55:2, 61-6.
More AW, Coke JM. Acute porphyric disorders. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;90:3; 257-62.
Fuad JM, Ali HA, Quraishi AM. Congenital erythropoietic porphyria (Gunther's disease) presenting as anterior staphyloma and blindness. JK-Practitioner 2001; 8(4): 262-264.
Neville B, Damm DD, Allen CM, Bouquot JE. Oral and Maxillofacial Pathology. W.B. Saunders Co. Philadelphia 1995.
Nancy W. Burkhart, BSDH, EdD, is an adjunct associate professor in the department of periodontics, Baylor College of Dentistry and the Texas A & M Health Science Center, Dallas. Dr. Burkhart is founder and co-host of the International Oral Lichen Planus Support Group http://www.bcd.tamhsc.edu/outreach/lichen/ and coauthor of General and Oral Pathology for the Dental Hygienist. Her Web site for seminars is www.nancywburkhart.com.
Past RDH Issues