Dental tourism

Is the risk of ‘foreign’ dental treatment worth the savings?
by Marcy Ortiz, RDH, BA
Traveling for medical procedures to third-world countries is not uncommon these days. A patient can receive a vast array of surgeries and treatments such as liposuction, general cosmetic surgery, fertility treatment, extensive orthopedic surgery, cancer therapy, and much more. The savings are substantial; for example, a particular website quoted a savings of up to 85% compared to the same medical care in the United States.1 Countries advertised as destinations for medical tourism include Poland, Belgium, Spain, Costa Rica, Argentina, India, Thailand, Malaysia, and Mexico (which is a popular destination).1

Google Maps offers this viewpoint of dental storefronts in Los Algodones, Mexico. The U.S. border lies just behind these offices.
Medical care is not the only reason for patients to seek a tourist vacation to the above destinations. A tourist can seek out dental care too, and, like medical tourism, Mexico also is a top destination. A patient seeking dental care can work directly with a tour company that provides a “travel agent” or adviser who plans the entire trip — flight, hotel, dental appointment coordination, and even airport transfers.
Dental tourism is a newly minted term for patients getting their dental work in foreign countries (usually third-world countries) while enjoying a vacation of sorts. It has become a big business. Dental offices do not routinely have patients leaving their practice to fly to Europe or India; however, Mexican dental tourism is a draw for Americans, combining a warm vacation with dental treatment.
American dentists and dental hygienists are not uniformly affected by dentistry offered in places like Mazatlan, Cancun, or Mexican border cities; however, dental professionals in Arizona, for example, understand the effects of dental tourism all too well. Arizona borders Mexico and is only a short drive away; American dental professionals routinely see new and current patients of record request follow-up treatment with a mouthful of dentistry performed by dentists in Mexico.
Although some Mexican dentists are trained in the United States, the majority are educated and trained in Mexico. They open their practices near border cities with the intent of competing with American dentists for patients. Years ago, this occurred only rarely, but with the recent economic downturn, patients take their diagnosed restorative needs from American offices and head south.
Arizona is not the only southwestern state affected by dental tourism. California and Texas are also affected. The corresponding U.S./Mexico border cities offering dentistry and pulling U.S citizens south is Tijuana (south of San Diego, Calif.), Juarez (south of El Paso, Texas), and Los Algodones (south of Yuma, Ariz.).
Patients who use these areas for dentistry can be creative, even deceptive, in how they use us to get a reliable diagnosis and merely take the tooth numbers and recommendations with them to Mexico. In the Arizona office where I work, we treat all patients as if they will consider us for their restorative treatments; but the majority of patients who travel to Mexico are brazen about jotting down the teeth we diagnose and taking the information with them. With these patients, our office is a place for current X-rays, prophylaxis, and a reliable diagnostician.
Who’s a dental tourist and why
The majority of patients called “dental tourists” who visit U.S. border offices for dentistry are Americans. In Los Algodones, 90% of the patients are American citizens.2 This hub is a massive retail experience for patients looking for dentistry. Los Algodones consists of only 4,000 residents but contains blocks of dental offices with at least 350 dentists. “The four square blocks of Los Algodones is said to be occupied by more dentists than anywhere else in the world.”2
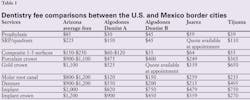
Lured by advertising, Americans seek out a variety of care in border towns such as Los Algodones. It is a one-stop place to purchase not only needed dentistry, but also medication and eyewear. The obvious reason is to save money. The savings can be staggering compared to the prices charged by U.S. dental offices, as most services are about two-thirds less than the price charged in large cities in Arizona (see Table 1). Crowns in metro Phoenix range from $800-900+, but in Mexico they are in the $200-300+ range, depending on the city and dentist visited.
Using simple arithmetic, we can see how a dental tourism trip can save thousands. For example, a husband and wife travel to Mexico; he needs three crowns, and his wife needs a crown and bridge. The average amount of savings for this couple is $3,600, ($6,300 fee in Arizona compared to $2,700 in Algodones). This savings is without consideration for cost of travel or lodging, if required.
While the above example may not seem substantial enough to travel to Mexico for dental care, it can be especially tempting when extensive work is required. A printed testimonial from a couple who traveled to Mazatlan for dental care stated, “My wife and I needed $21,472 worth of dental work to be done in the U.S. We got it done in Mazatlan for $3,500. We saved a mind-boggling $17,972.”3 Even by Mazatlan standards, this savings seems a bit overstated. Not mentioned is the specific diagnosed dental work by the U.S. dentist compared to what was actually completed in Mazatlan. Was it the same work? Less than what was diagnosed by the U.S. dentist? We do not know and neither does the couple; however, the primary factor for dental tourism is the savings, and this couple was very pleased with their “mind-boggling” dental savings.
Why is dental care in Mexico so economical compared to dental care in the United States? The reasons are many. First, the most obvious is Mexico has a lower cost of living than the United States; thus it is less expensive to live, open, and operate a business in Mexico. Mexican dentists do not have the expense of malpractice insurance, and their student debt is substantially lower than what a U.S. dental student incurs from attending a U.S. dental school. Mexican border dentists gear their practices toward Americans; thus, their practice is primarily a cash operation with little insurance to file for services rendered. Finally, what is most critical for patients considering dental tourism is the lack of regulations. Savings can be significant for a dental business owner without preoccupation of a government regulatory agency acting on behalf of the patient and employee regarding work environment, safety, or infection control.
Dental tourism marketing
Research of dental tourism reveals that the marketing is impressive. It is easy to see how the uninformed patient can be lured in search of reduced fee dentistry, despite a third-world country providing the service. The websites have professional appearances, fees are listed for specific services, accommodations, flights, tourist attractions in the area, travel agents, and some include pictures of staff with corresponding credentials.
All the offices contacted were quite diligent in responding to questions from a potential patient. My e-mails, sent to various offices in all three-border locations, were returned within the business day. One particular office continues to send follow-up e-mails on a weekly basis, asking if they can schedule dental work or answer any additional questions. Another office asked additional restorative questions in a professional manner regarding the condition of the tooth in order to provide a more accurate quote: does the tooth have a buildup, does it need a post, and what work if any has been performed on the tooth?
Included in the marketing is customer service styled like a vacation; the service is offered free of charge. One dentist in Tijuana, for example, offers a systematic procedure for ease in crossing the border: call us before you cross; we will be waiting for you on the Mexican side; you will be safe as we accompany you directly to the dental office for your appointment. Patients welcome this service because they feel safe having someone familiar with Mexico accompany them directly to their destination.
A competing Tijuana dentist offers multiple services in an attempt to get patients to this office. “We can arrange to pick up patients at the San Diego Airport ... we have a free shuttle from the border; just call us before you cross; we can help you with hotel reservation, and will pick you up at your hotel for your dental appointments.”4
The best accommodation offered through advertising is a shuttle service via chartered vans that originate from a Algodones dental office. Their chartered vans offer several services. First, they can pick you up on arrival at the airport. Second, they can transfer you from the American side of the border on the Yuma side, escorting you over the border and directly to the office. Finally, they offer a shuttle, customized and scheduled to pick up patients near a major Arizona city such as the greater Phoenix area. On the day of your service, they arrange for a guide to meet you at a “predetermined, Phoenix-area pick-up location. Sit back and enjoy the short ride to Mexico in [one of their] comfortable chartered vehicles.”5 This Mexican dental office is picking up Americans virtually in their own neighborhood without patients’ concerns of driving or getting into Mexico on their own. It is no wonder Americans, especially the elderly, are lured south for dentistry.
If tourism is part of the trip, there is an array of recommendations for places to go and things to do during the stay, especially if a long-term stay is required. For major crown and bridge, a dentist in Algodones requires a four-day turnaround for the finished product. This requires a return visit unless the patient plans a tourism trip staying the duration of time to allow for their more extensive dentistry and lab work to be completed. Photographs and video are included throughout the marketing process, focusing on the office, operatories, sterilizers, filtered water system, the dental staff, patient testimonials, and, of course, the savings patients experienced.
Testimonials are a popular way of influencing Americans to travel to Mexico and are easily provided using YouTube videos or similar format with actual patients describing pleasant experiences. In Tijuana, the testimonial message focuses on safety over the Mexican border by featuring elderly patients via YouTube commenting on how safe they feel while in Tijuana getting their dental treatment. “I was afraid before I came but I have had no problems…as far as safety over here, I feel safer here than I feel in areas of my own hometown.”4 This testimonial is potentially misleading by having an American assert that Mexican neighborhoods are safer than U.S. neighborhoods. I have traveled to many areas in Mexico, and I am aware there are places that you simply do not feel as safe as you do in the United States, especially after dark. This testimonial is a perfect example of misleading the public and shows how exaggerating the truth can be beneficial for financial gain in dental tourism.
Patients are not the only ones providing testimonials; there are quotes and recommendations by the dentists’ themselves on their dental websites. Some are a little rough in the translation. The wording in some of the advertisements was obviously misleading with intent of assuming quality or qualifications that are not accurate. The average patient will not see through this slight misinformation; however, the dental professional will.
A case in point is the advertising for a dental office in Algodones: “A Mexico border dentist usually receives similar standards of training as their U.S. counterparts;” “A Mexico border dentist is as good as or even better than those in other parts of the world.”5 A dental professional sees immediately that these statements are obviously misleading. “Receive similar standards of training” is not quite the same as an identical standard of training. The statement that their dentists compare or are better than those in other parts of the world may have some basis of truth if they are comparing only other third-world countries. Though not stated, a generalized statement of “other parts of the world” can imply inclusion of the United States in the comparison.
When border dental offices compete for American patients, the prime competition is with other dental offices in their location. If they can schedule a patient and get them to their office, this is money in their pocket vs. risking the patient choosing another office when they travel to the area unscheduled.
Once a “patient” arrives into the border city, hawkers bombard the tourists in hope of luring them to the specific office they are representing. Reputable dentists in Algodones call hawkers “jaladores, which means pullers.”6 The pullers are ultimate salespeople who do whatever it takes to get the person to their employer regardless of truth or ethics. Some jaladores may dress the part, wearing scrubs at the border for their sales pitch; others are walking advertisements by wearing signs and handing out cards; and some yell out that their dentist went to school at Harvard, even if it was only for a continuing education course.6
They may even degrade local dentists to gain business for their own employer. Not all dentists practice the jalador style business model. There is a group of dentists in Algodones who support change in the system of luring patients because the behavior is ethically wrong and gives tourists a poor perception of their city and business. However, a call for government intervention to stop this type of behavior has yet to occur.
What bothers U.S dentists who reside near these border dentistry cities is the Mexican dentists’ ability to advertise on the American side of the border. For example, Yuma is less than 10 miles from Algodones and the Mexican dentists advertise using the same methods as U.S dentists. One Yuma dentist resents the marketing and type of advertising he sees with Mexican dentists. He describes it as “predatory…you [go] across the border…they almost grab you and pass out cards. And they come across to Arizona and they advertise in our phone books, on our TV, and our radio.”6 “The problem with this ... Mexican dentists are not licensed to practice in the United States ... if they aren’t licensed here, they shouldn’t be able to advertise here.”6
Mexican dental tourism also advertises they will submit services rendered to American insurers for reimbursement. It is shocking to discover that dentistry in Mexico can be covered using U.S. dental insurance; however, our office stumbled upon this reality firsthand. Our experience involved a couple returning from Mexico after they had restorative work, a prophylaxis, and X-rays. They sought follow-up treatment in our office, and were patients of record, but were overdue according to our records.
Initially, we had no idea they had traveled to Mexico but we soon found out. We still did not know they had their dental insurance billed in Mexico and never considered it as a viable option; it was one detail our patients left out about their trip.
When our office billed their insurance for service rendered, we discovered they were just shy of being due for their six-month prophylaxis and were not due for X-rays. Their insurance declined payment to our office because they already paid the dentist in Mexico for treatment rendered within this six-month period.
Nonetheless, we were shocked that an American insurance company pays for treatment in Mexico. Our patients were upset because their insurance did not cover their visit at our office; the patients believed the insurance issue was our fault. Thus, they refused payment to our office on principle, and are now in collections.
Patient experiences
Many patients return to our office for their complete dental care after receiving restorative dentistry in Mexico. Most returning patients are vocal about their experience. Surprisingly, they are truthful about the positives, negatives, and their fears as well. Many patients are pleased with going to Mexico for the money they saved as opposed to actually understanding the condition of their dentistry. They return assuming the work is equal to U.S. standards. They are not sure, however, so they always ask for our opinion.
Some patients traveled with friends intending to receive dental treatment in Mexico, but changed their minds at the last minute. One patient, seen in our office for years, brought her Mexican dentist’s business card to enable me to refer others to a “good” dentist in Algodones. She was unaware that ethically I could never refer a patient to receive dentistry in Mexico. Below are actual dental tourism experiences from Arizona residents. Not all the patients had bad experiences, but some definitely regretted their decision.
Table 2Prevalent diseases in third-world countries (Mexico included)
Hepatitis A — transmitted through food and water
Hepatitis B — contracted through exposure to blood/infectious materials
Hepatitis C — viral infection contracted from blood contact through needles and medical exposure
Typhoid fever — Contracted through contact with feces, resulting effects are constant headaches. Mortality rate is 10%.
Amebiasis — water- or food-borne parasite resulting in intestinal illness, can affect blood, brain, and spinal cord
Shigellosis — bacterial infection found in water and food polluted by feces and contracted by hand-to-hand or hand-to-mouth contact. Mortality rate is 20% if untreated.
Tuberculosis — transmitted by the air, contracted through coughing, sneezing or sputum
Source: Trouble in Paradise: The untold story of dental tourism, brochure by Delta Dental of Arizona (2008)
• Example 1: This patient was from New Jersey, here for the winter, and presented with two broken posterior teeth. She made a trip to Algodones for medication and decided to have the crowns placed to save money. Upon returning to our office, the crowns appeared average or slightly above.
But when questioned, a few tidbits of information arose that were not all that surprising about her visit. The dentist required no medical history; absolutely no paperwork was required regarding the patient’s medical status or the fact that she requires antibiotic premedication. When I questioned her further, she stated she took the antibiotic because she knew better.
Not a single X-ray was taken, and the teeth were not evaluated for possible root canal treatment. When I asked, “What if the teeth needed root canal treatment?” she said that she guessed the root canal could be done after the crowns were placed if the teeth acted up.
• Example 2: A patient informed our office about having a problem with her new bridge recently placed in Mexico. She was in obvious discomfort. When examined by our dentist, he quickly saw the problem. Part of the patient’s cheek was cemented within the bridge placement. How the patient did not feel this before leaving Mexico was not clear. The patient never stated who cemented the bridge; a big assumption on our part is that the dentist was the one who cemented the bridge.
How a dentist or even a staff member can let a patient leave in this condition is shocking for us working in a high quality atmosphere. This patient was given two choices: our office would cut the bridge off, thus releasing the cemented cheek, and fabricate a new bridge, or she could return to Mexico for the original dentist to fix the mistake. She chose to return to Mexico.
• Example 3: A regular patient came in for his periodontal maintenance and it was obvious he had two implants placed since his last visit. When I questioned where he got the dental work, he said he had the implant surgery performed here in the United States (did not want to risk a surgical procedure in Mexico). To save money, though, he had the crowns placed in Mexico. While waiting for the crowns from the lab, this patient traveled to San Diego for a short vacation, returning a few days later to have the crowns seated in Mexico before returning back to Arizona.
Did this patient experience real savings? This patient merely spent the money saved on a short vacation, but in the end he was happy to have some fun in the sun while waiting for his implant crowns.
• Example 4: A patient lost a mandibular anterior tooth that required replacement. A single implant was recommended as the adjacent teeth were still in good condition. She decided to save money and get an implant placed in Mexico. The implant was placed, and an infection ensued. The new implant, along with two adjacent mandibular anterior teeth, were lost. Now the patient needs multiple implants, and at least three implant crowns or a bridge.
In this case, the patient did not save the money she anticipated; it actually cost her more financially and she endured additional pain and suffering from the poor implant care she received in Mexico.
Risks involved in dental tourism
Since money seems to be the primary factor for dental tourism, there are risks and standards that many patients are either unaware of or feel the risk is worth the savings. The foremost risk is the standard of infection control. In the United States, there are protections and standards in place to ensure optimal infection control and protection for patients receiving dental care. The agencies involved set and enforce these standards for U.S. dental practices. These agencies, boards of dental examiners and OSHA, require training and annual courses on the current infection control recommendations. They also require dental employees to receive the hepatitis B vaccine, which further protects the patient.7 These protections are not in place in Mexico. The patient receiving care there does not have the same assurance of patient safety or proper infection control.
For example, “More than 90% of U.S. dentists are vaccinated against hepatitis B compared to only 21% of Mexican dentists.”7 However, hepatitis B is not the sole risk due to lack of standards and regulation. Several infectious diseases are more prevalent in Mexico compared to inside the United States, such as hepatitis A, B, and C, typhoid fever, amebiasis, shigellosis, and tuberculosis (see Table 2). In fact, “hepatitis, tuberculosis, and typhoid fever are increasing at epidemic rates along the Mexican side of our southern borders.”7
Table 3Questions and considerations prior to dental tourism
- How will you determine the qualifications and experience of the dentist who will be treating you in a foreign country?
- How is payment processed?
- If you have dental insurance, will the benefits cover treatment that is performed outside the United States, and if so, to what extent?
- What happens if something goes wrong during or after treatment? Would you need to return to the country where you received treatment? Can you afford that?
- If you need corrective care after you return, will that be covered by your dental insurance or will you have to pay out of pocket for another dentist to provide corrective care?
- If something goes wrong after receiving dental care in another country, what are your legal rights?
Source: American Dental Association
U.S regulatory agencies requiring employee immunizations for hepatitis B alone has had a significant safety effect for employees and patients “particularly since standard precautions and routine vaccinations for dental workers were adopted (1985 and 1987, respectively). There have been no reported transmissions [of HBV, hepatitis B virus in the U.S.] from a dental worker to a patient since 1987.”8 The lack of sanitary conditions and regulatory infection control is a glaring problem in third-world countries and should be a serious consideration for Americans receiving dental work in a Mexican border city.
Another consideration is the training Mexican trained dentists receive compared to U.S. trained dentists. In the United States, there is the reassurance that “all American dental schools must be federally accredited. They offer the most highly skilled and technically advanced training, thus creating the most preeminent dental schools in the world.”7 Mexican dental training is not consistent compared to what dentists in the U.S. are required to perform and no uniform standard of care is in place. Without regulatory agencies, patients who encounter problems with their dentistry or health due to their procedures have “no legal or dental recourse in Mexico. [They] cannot file a complaint against a Mexican dentist and have the case judged by other dentists as [they] can in the U.S.”9
What ends up happening is obvious. The patient returns to the United States to have their problem fixed and repaired, whether it is botched dental work or a medical problem resulting from Mexican dental care.
Patients need to know their risks. As a result of more patients considering Mexican dentistry, it is imperative to review the questions and considerations outline in Table 3 with the patient before they undertake a trip for dental tourism. It may help them to reconsider and seek other options.
Safe alternatives
There are safer options for us to offer our patients who are considering a trip to Mexico or another third-world country for their dental care. First, introduce flexible alternatives in your office in an effort to keep patients here in the United States for their dentistry.
One option we offer our patients is an extended payment plan. This is especially helpful for patients who do not have dental insurance. Our office treats primarily geriatric patients and the majority does not have dental insurance. We have seen a positive response from our patients when they know they can make payments over a three-month period, without interest. This option enables them the opportunity to go ahead with their treatment plan. Others may respond to a cash discount or a senior-citizen discount when they do not have insurance.
Another consideration is to spread the patient’s restorative treatment over a longer period of time. This has been beneficial for many patients requiring extensive crown and bridgework that does not require immediate intervention. Simply treatment plan the most at-risk teeth and then complete a crown or two or one bridge each year. It is surprising how this makes the patient seem less overwhelmed compared to receiving a treatment plan in the tens of thousands of dollars. Of course, it may not be an option for serious dental decay, but for the more controlled patient with limited funds, it is a consideration.
A final option a patient may consider is to have needed restorative completed at a community-based dental clinic. This is for patients who simply cannot afford dentistry in a private practice dental office. In Arizona, community-based clinics are available but certain criteria limit accessibility, such as financial status, type of care, location, or long waiting lists for treatment. Some clinics restrict care to only children, low-income patients, veterans, or the homeless. One dental clinic for adults near our office has a three-year waiting list because the providers are volunteer dentists.
School settings are community-based options to consider for patients with a limited budget but plenty of time. Arizona has many dental hygiene schools but restorative options may be limited or may not be available. However, Arizona does have two new dental schools that offer reduced fees at 50% off usual and customary or more depending on the clinic. Reinforce to patients that all dental schools are required to have optimal infection control standards, licensed dentists who oversee their care, and costs are significantly less than in a typical dental office setting. If the patient has the time to devote to being a patient for the dental school, it may be a viable option.
It is our duty as dental hygienists to inform patients of the possible risks they may encounter when traveling to a third-world country for their dentistry. They need to know what these specific risks are as well as alternatives that are available for them to receive their needed dental work in the United States.
Provide your patients with the facts. Mexico has no regulatory agencies that ensure patient safety as the U.S does for its citizens. There is no standard to which Mexican dentists adhere. This is why dentists in Mexico can operate much cheaper. They do not have to pay their employees a living wage comparative to the United States, and there is no malpractice liability.
The savings are not worth the risks when receiving dentistry in a third-world country. Only after patients are aware and informed will they be better equipped to avoid the lure and pull of the clever marketing directed at Americans in an attempt to get them south of the border.
Marcy Ortiz, RDH, BA, has been a practicing dental hygienist for 24 years, the last 15 years in a geriatric dental practice in Sun City West, Ariz. She is a 2010 Arizona State University alumna graduating summa cum laude. She is a member of the Golden Key International Honour Society. She is the current vice president of education for Camelback Toastmasters in Glendale, Ariz. and was recently awarded 2010-11 Outstanding Area Y7 Toastmaster of the year. Marcy can be contacted at [email protected].
References
1. Find doctors around the world and save. All Medical Tourism. [Online] [Cited: September 26, 2011.] www.allmedicaltourism.com.
2. Salazar C. Los Algodones, Mexico, Has Become Dentist Capital of the World. Fox News Latino. [Online] January 19, 2011. [Cited: Aug. 12, 2011.] http://latino.foxnews.com/latino/health/2011/01/19/los-algodones-mexico-dentist-capital-world/.
3. Mexican Dental Vacation. [Online] [Cited: Sept. 27, 2011.] http://www.mexicandentalvacation.com/.
4. Sam Dental of Tijuana. [Online] [Cited: Sept. 23, 2011.] http://www.goodsamdental.org/.
5. Dayo Dental. [Online] [Cited: Sept. 13, 2011.] http://www.dayodental.com/articles-mexico-border-dentist.php.
6. Browne D, Joffe-Block J. Americans Head to Mexico for Cheap Dental Care: Insurance Industry Remains Somewhat Divided On Cross-Border Coverage. KPBS. [Online] Feb. 9, 2011. [Cited: Sept. 13, 2011.] http://www.kpbs.org/news/2011/feb/09/medical-maquila-insurers-are-following-americans-m/.
7. Delta Dental of Arizona. Trouble in paradise, The untold story of dental tourism: Dangers and risks of cross-border dentistry; Facts & issues: Delta Dental of Arizona, 2008.
8. Hepatitis B virus transmission in a dental office. Department of Health and Human Services for Disease Control and Prevention. [Online] 2011. [Cited: Sept. 15, 2011.] http://www.cdc.gov/mmwr/PDF/rr/rr5516.pd.
9. Griego R. Mexico dental care is a health hazard. The Arizona Republic. [Online] April 19, 2008. [Cited: September 10, 2011.] http://www.azcentral.com/arizonarepublic/opinions/articles/0419satlet3-191.html.
Dental tourism
Past RDH Issues