Health and wellness basics for the perio team
by Karen Davis, RDH, BSDH
[email protected]
I remember a time when I was updating a patient's health history form and the patient informed me of what their current cholesterol levels and blood sugar levels were. I felt insecure about how to respond, because I didn't remember what they were supposed to be! Were their levels high, low, or just right? I didn't remember.
This column is intended to be the resource I wish I had had years ago to post, review, and share with patients. Hopefully, it can be used to assist all of us in moving toward improved health and wellness choices based upon knowing current guidelines, and comparing them to where we actually are. The guidelines referenced are from the American Heart Association (AHA), American Diabetes Association (ADA), and the Centers for Disease Control and Prevention (CDC).
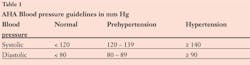
Let's start with the basics of blood pressure. If you are not currently providing a blood pressure screening on each patient prior to their dental visit, that is one service you can add immediately – it just might help save a life! Even though some states mandate that a blood pressure and pulse be recorded prior to dental procedures, it is still elective in most states. In my experience, I see that most dental professionals today are not yet in the habit of providing a BP screening prior to each visit. High blood pressure or hypertension is defined in an adult as a systolic pressure of 140 or higher and/or a diastolic pressure of 90 or higher. Table 1 shows the current AHA Blood Pressure Guidelines for Adults.
Do your current health history forms ask the patient to list their cholesterol and triglyceride levels? Perhaps they should, based upon a recent study published in the Journal of Periodontology that confirms higher lipid levels in patients with periodontitis compared to those without.1 Certainly, during our health history updates, we should encourage patients to have lipid panels updated with their physician if they are not aware of their cholesterol levels. Table 2 shows current AHA cholesterol and triglyceride guidelines.

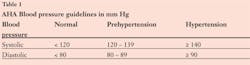
Does your current health history form ask the patient with diabetes to list their last HbA1c level? We now know that management of diabetes and periodontal diseases can be bidirectional, meaning that one condition can adversely or positively impact the other condition.2 If the blood glucose sticks to the red blood cells called hemoglobin, a chemical called HbA1c is formed. The percentage of HbA1c in the blood reveals what the blood sugar levels have been on average over the past two to three months. Knowing what a patient's HbA1C levels are prior to any type of periodontal treatment is important since periodontal infection may increase HbA1c levels, and treating the infection can make management of daily blood glucose levels easier.
Table 3 shows current ADA blood glucose and HbA1c guidelines.
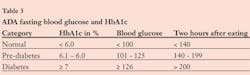
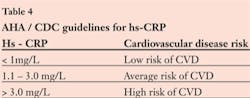
Should you have a patient in the chair who has chronic inflammatory conditions such as rheumatoid arthritis, cardiovascular disease (CVD), lupus, diabetes, periodontal disease, or suffers from obesity, their liver is likely producing a measurable increase in C-reactive proteins (CRP). This can be measured in the blood as a high sensitivity or hs-CRP level. CRP is an independent risk factor for cardiovascular heart disease.3 Table 4 shows current AHA/CDC CRP guidelines.
I'm pretty sure most current health history forms don't ask the patient to list their current body mass index (BMI), but given a recent study published in the Journal of Periodontology confirming positive associations between obesity and periodontal disease, perhaps we should consider it.4 Most patients either don't know what their BMI is, or don't know how to calculate it. So perhaps the role of the dental professional is to simply start there, in providing good information about overweight and obesity calculations and guidelines. Table 5 shows how to calculate BMI, and Table 6 shows current AHA BMI guidelines.
Lastly, a valuable resource that dental professionals can pass on to their patients as they increase their discussions about health and wellness is the American Heart Association's My Life Check website. This website easily assesses and calculates the risk of CVD on a scale of 1-10 using guidelines mentioned in this article. The web address is: www.mylifecheck.heart.org.

Be willing to calculate your own risk and encourage patients to evaluate theirs. By initiating conversations about basic health and wellness with patients, we have the potential to inspire change!
PerioTeam Takeaways
- Copy the tables listed in this article and share with every member of the team, as well as your patients who have any type of chronic inflammation.
- As a team, set good examples for your patients in the area of health and wellness by setting goals to reduce your own cholesterol, blood sugar, blood pressure, CRP levels, and BMI, as indicated.
- Complete your own and invite patients to complete the American Heart Association's My Life Check Calculator to determine current risk of CVD; then set goals to lower risks.
Karen Davis, RDH, BSDH, is the founder of Cutting Edge Concepts, an international continuing education company, and practices dental hygiene in Dallas, Texas. She is also a trainer for the JP Institute and serves on the Review Board for Dentalantioxidants.com. Her website is www.Karendavis.net.
References
1. Fentoglu O, Koroglu BK, Kara Y, Dogan B, et al. Serum lipoprotein-associated phospholipase A2 and c-reactive protein levels in association with periodontal disease and hyperlipidemia J Periodontol 2011;82:350-359.
2. Taylor GW. Bidirectional interrelationships between diabetes and periodontal diseases: An epidemiologic perspective J Periodontol 2009;80:1590-1598.
3. Ridker PM, Danielson E, Fonseca FA, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med 2008;359:2195-2207.
4. Chaffee BW, Weston SJ. Association between chronic periodontal disease and obesity: A systematic review and meta-analysis. J Periodontol 2010;81:1708-1724.
Past RDH Issues