Blinded by my sight
You know how you sometimes can't see something right in front of you? Oral cancer is like that. But screenings don't have to be that much of a hit-and-miss.
Recently, after a nice lunch, I went to the restaurant restroom and stood in the line that women so often experience. Two stalls for a restaurant that size just were not sufficient. I waited patiently while a mother with three young children attempted to take care of her personal needs - no easy task. The kids - being kids - punched, jumped, and played in the sink.
When one of the children ran behind me, I turned to see what would be the next mischief.
Lo and behold, there was another stall behind me that I did not see when I entered the restroom. My brain clouded my ability to see; I was blinded by my sight. How we see what we see is not only a function of our eyes, but also our brains. Improving vision means increasing what our eyes see and stretching our brains to interpret what is exposed.
This often happens with routine soft tissue oral cancer screenings; we make assumptions based on previous experiences, or we’re distracted and don’t see what’s there. Other times we just can’t see. Oral cancer is a disfiguring affliction that kills half its victims. In the past, it has been difficult to detect in its early stages, but this is no longer true. Using early detection options in addition to standard measures, oral health professionals can change this, yet we seem to resist the adoption of new options.
Where we are now
Long before there is overt disease breakdown, there are changes in a person. Statistics tell us we are not doing enough. A majority of oral cancers are still not being caught until Stage III or IV, with greater than 50 percent of victims dead in five years. This statistic has not significantly improved in 40 years!1-4
New early detection modalities have come to market, and more are on the way. Most professionals have heard about these early detection systems, yet only about 5 percent routinely use them. It’s been said everything is new in dentistry for 10 to 20 years. This may have been true and even acceptable in the past, but this is the 21st century and it’s time for more professionals to shift their thinking and update their thoughts and systems.
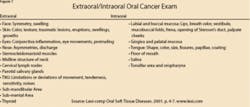
The standard for oral cancer detection remains the extraoral/intraoral soft tissue exam5 (see Figure 1), yet it is not the first step. The first step is risk assessment, including a thorough review of the health profile. The highest risk factors remain tobacco and alcohol, yet there are many other factors to assess. Though risk assessment sounds like a good idea, there is little consistency to our current application. A simple, easy-to-use, inexpensive risk assessment tool is available through PreViser Corporation (www.previser.com) - a validated computer-based system for quantifying risk for caries, periodontal disease and oral cancer.6-8
The PreViser tool takes data already gathered and places the individual into a risk category. Based on the categorization, the practitioner can make more consistent, objective, and accurate clinical decisions, can reduce the need for complex therapy, and can offer risk reduction modalities. But even with good risk assessment, the fact remains that 25 percent of oral cancer victims have no lifestyle risk factors. In the past three decades, an increase of 60 percent in tongue cancer was detected in people under 40.1-4

What has been the standard to this point is clearly not working well enough. Several options for earlier detection can help change these statistics. Each system can help increase awareness. Early detection modalities are not meant to replace standard screening but to improve its yield. (Figure 2 shows three early detection systems currently available).
HPV risk and new vaccine
Some good news is that tobacco consumption has dropped in the United States. The bad news is that the incidence of oral cancer has not correspondingly dropped. This information, along with the 25 percent of oral cancer cases with no known risk factors, caused researchers to look for new possible causes.17 Another risk factor now recognized is the human papilloma virus (HPV). HPV is a group of more than 100 viruses. Some types of HPV are associated with certain types of cancer, and these are called high risk oncogenic or carcinogenic HPVs.16
A June 2006 review by Fakhry and Gillson in the Journal of Clinical Oncology made the association even stronger. It said, “HPV is now recognized to play a role in the pathogenesis of a subset of head and neck squamous cell carcinomas, particularly those that arise from the lingual and palatine tonsils within the oropharynx.”18
The statistics on HPV are staggering. Approximately 20 million people are currently infected with HPV. Fifty to 75 percent of sexually active men and women acquire genital HPV infection at some point in their lives. About 5.5 million Americans get a new genital HPV infection each year.
In June 2006, the Advisory Committee on Immunization Practices (ACIP) from the Centers for Disease Control (CDC) voted to recommend first vaccine Gardasil®, which was developed to prevent cervical cancer and other diseases caused by certain types of HPVs. The vaccine is recommended as early as 11 to 12 years old, and can be given as young as nine.19 The vaccine does not treat existing HPV infections, genital warts, pre-cancers, or cancers, making risk assessment and early detection even more important.
The near future
The future continues to unfold with more options in research and the FDA (Food & Drug Administration) approval process. Researchers at the School of Dentistry at UCLA laboratories have discovered possible biomarkers in saliva for the detection of oral cancer, as reported at the American Association for Dental Research meeting earlier this year. Next, the Saliva RNA test will undergo clinical testing.9-11
The National Institute of Dental and Craniofacial Research (NIDCR) is making a concerted effort to lay the scientific groundwork for a new generation of oral cancer screening tools. In the March 2006 issue of Inside Scoop, NIDCR grantee Dr. Miriam Rosin, a senior staff scientist at the British Columbia Cancer Agency in Canada, said, “We thought of toluidine blue, a staining dye that has been used for decades to identify various tumors including oral cancer. Dentists are very familiar with it, and preliminary work from our laboratory and David Sidransky’s lab at Johns Hopkins shows that toluidine blue appears to differentially stain early precancerous lesions.”13,20
Extensive research has been done in this area, and soon there may be another FDA approved option called OraTest®, a patented five-minute mouthrinse that uses a stabilized and patented formulation of toluidine blue. OraTest is already approved in more than a dozen other countries.
ViziLite Plus was introduced at the American Dental Association Annual Session in October 2005.12 This system combines the oral screening technology of ViziLite with advanced chemiluminescent light technology and TBlue630, a marking system using Zila Tolonium Chloride™ (ZTC). ZTC is a patented composition designed to be superior to traditional toluidine blue. ZTC is the primary staining component in TBlue630 and OraTest, which is progressing through the regulatory process of the FDA.14 In December 2005, Zila began Phase III clinical testing, which can take a year or more.15 These are exciting times with so many new developments and options pending.
We don’t have to wait and shouldn’t hesitate when excellent adjunctive options are already available. With our increasing ability to reduce the horrendous mortality rates for oral cancer, it is unfortunate that adoption is relatively slow and inconsistent.
Are you vision driven?
Do you look at your schedule and see the same old thing? Can you think of one thing you’ve changed in the last year? One of the strongest assets human beings have is the ability to form habits. A downside to these habits is that one starts taking the path of least resistance. As professionals, we want to do what we know is best. We may change our behavior, but then autopilot kicks in, and we often fall back into old behaviors, even when they do not serve us well.
Can you imagine a world with no oral cancer? Early detection modalities are about visualizing what we can’t see and identifying areas that may be difficult to see. What is blocking our vision might be our inability to see lesions. Many people see a future they would like to see; yet few do anything to make it a reality. Become vision driven. Step up and be a leader in your practice. Attend courses on early detection and then go for it! As Mahatma Gandhi said, “We must become the change we want to see.” RDH
References
1. Cancer prevention, early detection, and prediction. National Cancer Institute. Available at http://www.cancer.gov/aboutnci/2015/cancer-Prevention-Early-Detection-and-Prediction. Accessed Mar 9, 2006.
2. Rates of occurrence in the United States. Feb 2006. The Oral Cancer Foundation Web site. Available at: http://www.oralcancerfoundation.org/facts/. Accessed Apr 13, 2005.
3. Head and neck cancer. Nov 2005. Oncology Channel Web site. Available at: http://www.oncologychannel.com/headneck/index.shtml. Accessed July 26, 2005.
4. What are the risk factors for oral cavity and oropharyngeal cancer? March 2006. American Cancer Society Web site. Available at: http://www.cancer.org/docroot/CRI/content/CRI_2_4_2X_What_are_the_risk_factors_for_oral_cavity_and_oropharyngeal_cancer_60.asp?sitearea=CRI. Accessed July 26, 2005.
5. Newland J, Meiller T, Wynn R, Crossley H. Oral Soft Tissue Diseases. 2001. Lexi-Comp. Hudson: Ohio. p.4-7.
6. Page RC, Krall EA, Martin J, et al. Validity and accuracy of a risk calculator in predicting periodontal disease. J Am Dent Assoc. 2002;133:569-576.
7. Page RC, Martin J, Krall EA, et al. Longitudinal validation of a risk calculator for periodontal disease. J Clin Periodontol. 2003;30:819-827.
8. Page RC, Martin JA, Loeb CF. Use of risk assessment in attaining and maintaining oral health [published erratum appears in Compend Contin Educ Dent. 2004;25:905]. Compend Contin Educ Dent. 2004;25:657-670.
9. Wong D. “Salivary diagnostics powered by nanotechnologies, proteomics and genomics” J Am Dent Assoc 2006 137: 313-321. Available at: http://jada.ada.org/cgi/content/abstract/137/3/313. Accessed Apr 25, 2006.
10. Shagat S. “UCLA School of Dentistry Researchers have standardized a saliva-based test for oral cancer, ushering in an era of new possibilities for cancer detection” UCLA News. March 9, 2006. Available at: http://newsroom.ucla.edu/page.asp?RelNum=6883 Accessed Apr 25, 2006.
11. Malamud D. “Salivary diagnostics: The future is now” J Am Dent Assoc 2006 137: 284-286.
12. Zila to Launch ViziLite(R) Plus TBlue630TM at Annual ADA Meeting. Business Wire; 10/5/2005. Available at: www.highbeam.com/library/docFree.asp?DOCID=1G1:137135123 Accessed July 31, 2006.
13. Bringing the promise of molecular medicine to oral cancer screening. Inside Scoop, National Institute of Dental and Craniofacial Research. March 2006. Available at: www.nidcr.nih.gov/NewsAndReports/Media/InsideScoop3162007.htm. Accessed July 31, 2006.
14. Ozols J. Healthy Mouths. Newsweek. Dec 22, 2005. Available at: http://msnbc.msn.com/id/6746583/site/newsweek/print/1/displaymode/1098/ Accessed June 17, 2006.
15. Zila Begins Phase III OraTest(R) Clinical Trial with Investigators’ Meeting. Healthcare Sales and Marketing Network. Dec 13, 2005. Available at: http://salesandmarketingnetwork.com/news_release.php?ID=2009008. Accessed June 17, 2006.
16. Human Papillomaviruses and Cancer: Questions and Answers. June 8, 2006. National Cancer Institute. Available at: http://www.cancer.gov/cancertopics/factsheet/Risk/HPV Accessed June 17, 2006.
17. Waldman H. Vaccine Treatment Takes Aim At Oral Cancer. June 6, 2006. UConn Health Center. Available at: http://cancer.uchc.edu/news/releases/oralcancer.html Accessed June 17, 2006.
18. Fakhry C, Gillison M. Clinical Implications of Human Papillomavirus in Head and Neck Cancers J Clin Oncol 2006 24: 2606-2611 Available at: www.oralcancerfoundation.org/facts/humanpapillomavirus.htm Accessed Aug 2, 2006.
19. HPV Vaccine Questions and Answers. June 2006. Centers for Disease Control. Available at: http://www.cdc.gov/std/HPV/STDFact-HPV-vaccine.htm Accessed Aug 2, 2006.
20. New oral test detects genetic alterations predictive of oral and head and neck cancers. 2001. Abramson Cancer Center University of Pennsylvania. Available at: http://www.oncolink.com/resources/article.cfm?c=3&s=8&ss=23&id=1472&month=07&year=2001 Accessed June 17, 2006.
Patti DiGangi, RDH, BS, is a speaker, author, and practicing dental hygienist who offers CE courses to national audiences through her company, Professional Direction Conferences. Courses are on eagle eye dental hygiene assessments, minimal intervention, the perio/systemic link, dental benefits, and early oral cancer detection. She can be reached at [email protected] or (630) 292-1473.