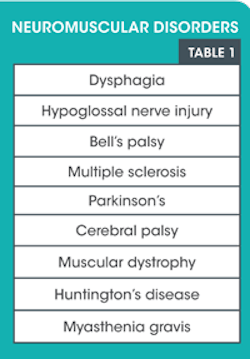
Neuromuscular disorders affect the oral cavity
The impact on oral hygiene procedures should be monitored
by SHERI B. DONIGER, DDS
Several neuromuscular disorders will affect the oral cavity. As a dental hygienist, you are the initial line of defense for the dental team. You see the patient first and note all variations during the intra- and extraoral examination. As dentition, soft tissues, and occlusion may be permanently affected by several of these conditions, the dental hygienist is integral in collecting data for the diagnosis and management of these conditions.
All patients fill out a health questionnaire prior to their first visit. Some forms are more robust than others. As with any questionnaire,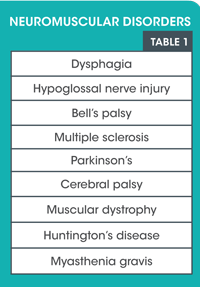
Certain sequellae may appear to affect the ability to swallow. Radiation therapy and some drugs may cause xerostomia that may appear to be neuromuscular in nature, but is symptomatic, not organic. Other conditions may mock true neuromuscular disorders. Hypoglossal nerve injury may be caused by an errant anesthetic needle, a tumor at the base of the brain, a stroke, cellulitis, or an infection. On the other hand, the hypoglossal nerve may also be injured by any diseases that affect motor neurons, such as Huntington's disease, amyotrophic lateral sclerosis (ALS), or Parkinson's, which we will discuss later. Paresthesia may also exhibit symptoms similar to neuromuscular disorders. Both will exhibit signs of tongue paralysis and difficulty in speaking, chewing, or swallowing.
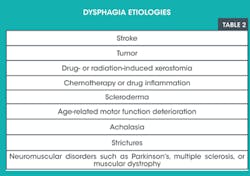
Swallowing, as we know, is a multisystem event. It involves proper musculature and nerve transmission to the brain, as well as assistance by the teeth in mastication and the salivary glands in lubrication and enzymatic action on food. Furthermore, it will be affected by any issues affecting the larynx or esophagus. Dysphagia, or difficulty swallowing, usually affects older adults although it can also affect babies. Forty percent of nursing home residents are affected by this malady. Dysphagia has many etiologies. Some of the more common causes are listed in Table 2. Dysphagia may be caused by an actual blockage, such as GERD (gastroesophageal reflux disease) or the inability of the muscles to conduct peristalsis due to an underlying neurological disease such as muscular dystrophy, Parkinson's, or multiple sclerosis. Patients with dysphagia will exhibit symptoms of difficulty swallowing, may have issues with chewing due to lack of swallowing function, or have problems moving food from their mouth and through their esophagus. They may feel as if they have a lump in their throat. They may also exhibit malnutrition, dehydration, as well as aspiration of food particles due to coughing and choking as they try to clear their esophagus.
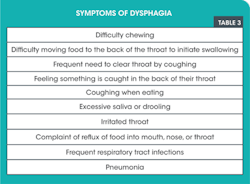
These patients need to be seen by their physician to determine the etiology of their swallowing dysfunction. We may see them before they realize they have a swallowing issue. We may notice food and materia alba buildup on the tooth surfaces as well as noncleared food from the oral cavity. Patients may exhibit frequent dry coughing or attempts to clear their throat at times not surrounding meals. Table 3 lists a group of potential symptoms from patients who experience dysphagia. These patients may have underlying neuromuscular issues. It is definitely a starting point to have a discussion about their ability to swallow.
Bell's palsy as well as hypoglossal nerve injury may be caused by a dental injection or a tumor. Both will have an effect on the patient's condition. Both may be temporary or longer lasting, depending on the etiology. With Bell's palsy, which affects the seventh cranial (or facial) nerve, only one side of the patient's face is affected. There may be a rapid onset of mild weakness to a full-blown facial paralysis. Facial expression may be affected by the weakness of the muscles, in addition to a sensation of pain or increased sensitivity on the affected side. Headaches are not uncommon. Taste may be affected. Lyme disease or herpetic lesions may also cause Bell's palsy.
The twelfth cranial nerve, which controls tongue movement, is the hypoglossal nerve. Hypoglossal nerve injury is also usually unilateral, with the tongue deviating to the affected side. Unilateral atrophy of the tongue may be a sign after prolonged injury to this nerve. Etiology of hypoglossal nerve injury may also be caused by tumors, stroke, or any of the degenerative diseases affecting muscles and nerves. Patients will have difficulty speaking, talking, and chewing with both of these conditions. Oral hygiene may be affected as well as oral clearance.
Multiple sclerosis is a disease of muscular control, affecting more women than men, usually diagnosed between the ages of 20 and 40. It is a degenerative disease, caused by inflammatory damage to the nerve sheath, exhibiting muscle weakness over time. Patients may exhibit delayed motor skills, drooling, ptosis, tremors, lack of balance, and lack of motor control. Some facial paralysis may develop and affect the ability to perform proper oral hygiene procedures and may affect the ability to retain removable prostheses.
Parkinson's usually develops in patients after the age of 50, affecting men and women equally. It is caused by a continual breakdown of neurons in the brain, decreasing the dopamine and decreasing muscular function over time. These patients exhibit tremors as well as muscular stiffness. Drooling, muscle aches, muscular atrophy, and difficulty swallowing are also signs. The tremors and inability to keep their mouths open may cause a challenge to receiving dental care. Some Parkinson's medications will affect saliva as well as blood pressure. Special care will be required in managing these patients.
Cerebral palsy affects both the brain and the nervous system, and it may be manifested any time from early infancy. It is due to an injury or abnormality in the brain. This usually does not get worse over time. Different types of cerebral palsy exist and patients may exhibit a variety of symptoms. Patients may exhibit tremors, muscular and joint tightening, an unsteady gait, and weak musculature. Patients with cerebral palsy may exhibit more malocclusion, bruxism, and hypocalcification, as well as oral injuries caused by falling due to concomitant muscular issues. Some of these patients may be on antiseizure medication, which has the potential to affect gingival growth.
Muscular dystrophy is a genetic condition that exhibits loss of muscle tissue, leading to muscular weakness, which worsens over time. Affected muscles may be localized (pelvis, shoulder, or face) or may be more widespread throughout the body. There are several types of muscular dystrophy. Myotonic will affect chewing and the ability to move lips and turn one's head. Patients may experience malocclusion and TMD due to the muscular weakness.
Huntington's disease may exhibit uncontrollable movements due to nerve cells in certain parts of the brain degrading and degenerating. It is a genetic defect of chromosome four, which causes a section of DNA to repeat several times. Patients tend to develop symptoms between the ages of 30 and 40, but, rarely, it may occur in younger children or adolescents. Patients may exhibit unusual movements including grimacing, head turning, abnormal gait, and wild movements of the extremities. They also lack muscular control of the face and tongue. Swallowing is also an issue. Oral hygiene may be quite difficult due to the uncontrollable movements.
Myasthenia gravis is an autoimmune neuromuscular disorder. The etiology is unknown but it may be due to a tumor of the thymus. It can occur at any age though it is more common in young women and older men. Patients experience partial or no facial expressions because of facial paralysis. These patients have muscle weakness in their tongues as well as palates, making swallowing and chewing difficult. Patients may also experience breathing difficulties due to weakened muscles of the chest wall, as well as a droopy head.
These disorders are by no means a complete list. There are always untoward reactions to medications or disease states that may cause issues with the oral cavity. Xerostomia due to medications or aging may cause symptoms that mimic neuromuscular diseases. Some senior patients may exhibit symptoms of xerostomia, slight tremors, and lack of dexterity or slowness in gait without a concomitant neurological or muscular-based disorder. These may be components of the normal aging process.
As with all of the listed issues, care will need to be moderated to ensure patient comfort. Potential solutions may include shorter appointment times, sedation, or general anesthesia. Sometimes sedatives may worsen the patient's condition. It is wise to be in concert with the general practicing physician for these (or any) patients to confirm any medicine interactions. Patients with mobility issues may need assistance entering and exiting the treatment chair. Depending on the severity of the patient's conditions, procedures may need to be modified due to the patient's level of comfort and ability to sit for the procedure. Pillows may be needed for extra comfort. Bite blocks may be utilized to prevent unexpected closure due to uncontrolled neurologic responses.
Changes in medications and current dosages should be noted at every appointment. It is paramount for both the business manager (first contact in the office) as well as the dental hygienist to confirm any changes in medical condition and medications prior to the start of any dental treatment.
Oral hygiene modifications may be necessary, and caregivers may need to be given instructions if patients are not capable of performing the task by themselves due to physical limitations. As a hygienist, you must always be mindful of patients' abilities and consistently have suggestions and options for their oral care. These may need to be altered over time. Your outstanding care will help improve their general health by maintaining their oral health. RDH
References
Dysphagia:
http://www.webmd.com/digestive-disorders/tc/difficulty-swallowing-dysphagia-overview Accessed Dec. 23, 2012
Muscular dystrophy:
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002172/ Accessed Dec. 23, 2012
Multiple sclerosis:
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001747/ Accessed Dec. 23, 2012
Parkinson's disease:
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001762/ Accessed Dec. 23, 2012
Cerebral palsy:
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001734/ Accessed Dec. 23, 2012
Muscular dystrophy:
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002172/ Accessed Dec. 23, 2012
Huntington's disease
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001775/ Accessed Dec. 23, 2012
Myasthenia gravis:
http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0001731/ Accessed Dec. 23, 2012
Sheri B. Doniger, DDS, has been in the private practice of family and preventive dentistry for more than 20 years. A dental hygiene graduate of Loyola University prior to receiving her dental degree, her current passion is focusing on women's health and well-being issues. She may be contacted at (847) 677-1101 or [email protected].
Past RDH Issues