Understanding How Motivation Achieves Patient Compliance

Dental hygienists must understand the basic concepts of human motivation before they can help patients achieve their goals.
Every day, dental hygienists are in a position to help patients improve their oral and systemic health. The success of these professionals, and the health of their patients, is based on the hygienist’s knowledge and skills regarding patient motivation and education. It is essential that hygienists understand basic motivational theories and concepts to determine which approach will be successful for each patient.
As members of a helping profession, dental hygienists deal with compliance issues to help patients achieve optimal oral and systemic health. To obtain compliance, existing behaviors must be altered. Whether hygienists want compliance in the area of oral health, weight loss, tobacco cessation, or high blood pressure reduction, they must understand the basic concepts of human motivation before they can help patients achieve their goals. This article discusses types of motivation, theories and components of motivation, and motivational concepts. It provides a better understanding of human behavior, and enough information regarding these topics to help hygienists gain a higher level of patient motivation and compliance.
According to Franken (2002), there are two types of motivation: avoidant and approach. The avoidant type causes people to choose certain behaviors in order to avoid something. In contrast, the approach type causes people to be driven by want or need. For example, if a person wants to lose weight, he or she may choose the avoidance approach by avoiding desserts. The person realizes avoiding high calorie foods can result in weight loss. However, in the approach method of motivation, the individual may choose to exercise more, realizing that burning extra calories will result in weight loss. People who are anxious are more likely to engage in avoidant behavior (Franken, 2002) and are typically introverts. Franken says that not all people are equally anxious. Some are anxious from birth. On the other hand, people who are less anxious tend to be more extroverted and seem to be driven by approach behaviors. People may use a combination of approach and avoidance to achieve the desired result.
Goals and rewards
Motivational psychologists have developed theories of motivation or behavior. Two of interest to dental hygienists trying to motivate patients are the reward theory and the goal theory. The reward theory says people repeat behaviors that make them feel good (positive reinforcement) and discontinue behaviors that make them feel bad (negative reinforcement) (Franken 2002).
The goal theory says that goals give rise to actions (Locke & Latham 1990). According to this theory, goals create tension and people work toward the goal to reduce that tension (Franken 2002).
It is easy to understand how hygienists can motivate through the reward theory. They can offer positive and negative reinforcement based upon patients’ performances. For example, if during a routine recare visit the hygienist discovers a patient’s blood pressure is high, it’s appropriate to discuss whether the patient is taking his blood pressure medication, if he is watching his diet, and if he is exercising. At the next visit, if the hygienist discovers the patient’s blood pressure is lower, it is a great opportunity to provide praise. This positive reinforcement will make the patient feel good and likely continue the behavior that lowered the blood pressure. On the flip side, if the patient’s blood pressure is still elevated, there should be discussion and questions regarding medication, diet, and exercise.
In regard to the goal theory, where do the goals come from? This can be answered by what Franken refers to as the components of motivation (Franken 2002). He contends that goals arise from three components: biological processes, learned processes, and cognitive processes.
Think about the patient with high blood pressure. The biological component of the high blood pressure may be due to the need to eat. When he is stricken by the need to eat, the foods he consumes may play a part in the high blood pressure. Any genetic links to high blood pressure are also biological components - those that “hard wired” in our brain and body’s systems. Several learned components may also contribute to high blood pressure, such as consuming fast food and leading a sedentary lifestyle. The cognitive component of the patient comes into play when he decides, based on new information, that these habits are not beneficial to his health and he changes his behavior. The hygienist’s main role is to educate patients by providing information that can facilitate changes in the cognitive component.
Two other theories of motivation that are important for hygienists to consider are internal and external motivation. Patients who are intrinsically motivated undertake an activity for its own sake (Mark Lepper 1988). These people have an internal drive that is self-generated, and they don’t need much motivation from hygienists to attain the desired goal.
Externally motivated patients want to obtain a reward or avoid some punishment external to the activity (Lepper 1998). These patients depend on feedback from hygienists, such as praise, or a visible result, such as lower blood pressure or aweight loss. Extrinsic motivation can be short-lived. Establishing if patients are intrinsically or extrinsically motivated can help hygienists determine how much feedback patients require.
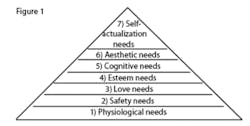
In order to be effective motivators, hygienists should understand Abraham Maslow’s need theory. He said that basic physiological needs are associated with deficiency, and the higher order needs are associated with growth. He arranges categories in a hierarchical fashion with basic needs at the bottom (see Figure 1). Patients can only advance to the next category when the category before it has been fulfilled.
For example, say a patient has no home and has spent months on the street. If he visits the dental office with a toothache and his mouth is full of plaque, Maslow’s need hierarchy states that no matter what the dental staff does in the way of education, that patient is not going to comply until he advances up the pyramid to the fifth stage, which is cognitive needs. It is important to recall Maslow’s pyramid when trying to determine affective ways to motivate patients.
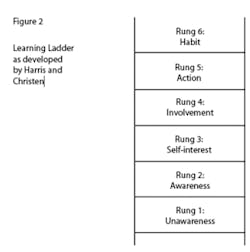
Another tool that is beneficial to dental hygienists is the learning ladder (Harris & Christen 1995). Through the learning ladder, patients progress from unawareness to habit (see Figure 2). To demonstrate the ladder, imagine a patient who does not floss daily. When the patient arrives at the dental office, she is on the bottom rung, the rung of unawareness. The dental hygienist has the obligation to educate and motivate this patient into daily flossing to achieve optimal oral health. The patient typically will not progress to the top rung of the ladder in one or two hygiene visits, but through regular visits and consistent guidance.
There are some qualities dental hygienists should possess that Harris and Christen consider tools of motivation. These are having an in-depth knowledge of health issues concerning patients, being able to understand patients’ situations, being considerate of patients, and being able to talk with patients so they can understand (Harris 1995). When dental hygienists use these qualities, patients stand a better chance of successfully reaching their goals. Hygienists who do not possess an in-depth knowledge cannot effectively educate patients, thus patients cannot move up the learning ladder to the second rung of awareness.
These research findings can be valuable to hygienists who take the time to learn and understand them. There are many issues to consider when trying to gain patient compliance through motivational strategies. What appears to be teaching patients the “how-to’s of brushing and flossing” becomes an in depth process, one involving understanding each patient so that motivational strategies can be personalized. RDH
References
Cronenberger, J. (1995, May). Motivating grumpy, sleepy and bashful. Registered Dental Hygienist, 32-37
Franken, R. (2002). Human motivation (5th Ed.). California: Wadsworth.
Gluch-Scranton, J. (1991, July). Motivational strategies in dental hygiene care. Seminars in dental hygiene, 1-6
Harris, N. & Christen, A. (1995). Primary preventive dentistry. Connecticut: Appleton & Lang.
Student motivation to learn. (n.d.). Retrieved March 10, 2005, from http://www.kidsource.com/kidsource/content2/Student _Motivation.html
Weinstein, W. (1997). Helping patients change their oral self-care. Dental Hygiene News, 6(2), 16-19.