Neurilemmoma: Histological exam needed for diagnosis of the tumor

By Nancy W. Burkhart
The neurilemmoma arises from the proliferation of the neural sheath's Schwann cells of the peripheral cranial, spinal, and autonomic nerves. The tumors are usually found in the head and neck region. Other names for the neurilemmoma include schwannoma, perineural fibroblastoma, and neurinoma.
Oral and perioral manifestations may occur in the soft tissues of the mouth, the tongue, and, on rare occasions, the lip area (see Figure 1). Additionally, some of the tumors may occur in intraosseous regions but are less common in the palate, gingivae, floor of the mouth, and buccal mucosa. However, Kudoh et al. (2015) reported on a neurilemmoma described as a soft, dome-shaped, sharply circumscribed, localized, tumor mass in the hard palate region that measured 3.0 cm. The tumor was thought to arise from the greater palatine nerve. Additionally, Rathore et al. (2015) reported a similar size tumor in the retromolar region of a patient. Lambade, et al. (2015) reported on a case study involving a schwannoma of the cheek. Therefore, the size and location of the neurilemmoma may vary.
A related tumor occurs with similar clinical appearance and this is the neurofibroma. Schwann cells occurring in the neurilemmoma must be differentiated from a diagnosis of a neurofibroma. When a neurofibroma occurs, neurofibromatosis (Von Recklinghausen disease) is a consideration in a differential diagnosis and is of clinical significance. Normally, the neurilemmoma is a solitary lesion, and there may be multiple neurofibromas with regard to neurofibromatosis.
Generally, a neurilemmoma occurs in an age range of 20 to 50 years of age and may occur in both male and female populations. The tumor is very slow growing, usually asymptomatic and typically will reach .5 to 1 cm in size. Some neurilemmoma tumors may be very fast growing, and this may lead to the consideration of other types of malignant tumors in a differential diagnosis. Proliferation of the Schwann cells causes a fibrous capsule to form around the tumor. The nerve is pushed aside as the tumor continues to grow and may produce dull sensations, pain, and/or paresthesia, especially when they occur in bone.

Figure 1: DeLong L, Burkhart NW. General and Oral Pathology for The Dental Hygienist. 2nd Ed. 2013; Wolters Kluwer Health: Lippincott Williams & Wilkins, Baltimore.
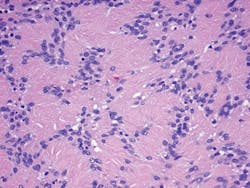
Figure 2: Histology of a neurilemmoma (Courtesy of Dr. Harvey Kessler). The classic Antoni A pattern of the neurilemmoma is depicted in the image. Note that the spindle cells appear in a palisade or whirling appearance with whirls and waves throughout the specimen.
Histology confirmation-The histology confirmation is instrumental in the diagnosis of the tumor and also in the differentiation of other types of tumors. Microscopically, the neurilemmoma is a mass of spindle-shaped cells surrounded by a fibrous capsule composed of residual nerve fibers and the connective tissue that forms the support structure for the peripheral nerves.
The spindle cells appear in a palisade or whirling appearance with whirls and waves throughout the specimen. Two patterns are possible, Antoni A and Antoni B. Both have varying degrees of patterns with regard to the arrangement of the cells. The pattern of elongated spindle-shaped cells with nuclei are palisaded or regimented around eosinophilic bodies (Verocay bodies) to produce a distinct appearance in the Antoni A pattern depicted in Figure 2. Antoni B pattern is less cellular and regimented with fewer palisading distinctions and haphazard arrangement. The tissue will also express S-100 protein in the immunohistochemistry.
Differential diagnosis-Histological examination is needed for a diagnosis.
• Neurofibromas (lacks the thick collagenous capsule of a schwannoma)
• Leiomyoma
• Traumatic fibroma
• Traumatic neuroma
• Lipoma (the lipoma is usually softer with a yellow hue)
Radiographic and clinical appearance-The radiographic appearance is that of a well-defined radiolucency. Neurilemmoma lesions are generally found within tongue tissue, but, when they occur in bone, the maxilla or mandible may be affected. The tumor is usually seen clinically as a solitary smooth, firm nodule within the head and neck region. The tumor may also be found in other areas of the body such as the flexor surfaces of the arms and legs.
The treatment for a neurilemmoma is surgical excision. The recurrence is rare and the prognosis is excellent. Because some tumors are discovered at a later stage, the amount of tissue that must be removed could be extensive depending upon the size and amount of destruction. Early diagnosis and intervention is key.
As always, continue to ask good questions and listen to your patients! RDH
References
1. DeLong L, Burkhart NW. General and Oral Pathology for The Dental Hygienist. 2nd Ed. 2013; Wolters Kluwer Health:Lippincott Williams & Wilkins, Baltimore.
2. Kudoh M, Harada H, Matsumoto K, Sato Y, Omura K, Ishii Y. Massive neurilemmoma of the hard palate in which preoperative diagnosis was difficult. Hindawi Publishing Corporation Case Reports in Surgery Volume 2015, Article ID 638025, 8 pages http://dx.doi.org/10.1155/2015/638025.
3. Lambade PN, Palve D, Lambade D. Schwannoma of the cheek: clinical case and literature review. J Maxillofac Oral Surg. 2015 June; 14(2): 327-31.
4. Rathore AS, Srivastava D, Narwal N, Shetty DC. Neurilemmoma of retromolar region in the oral cavity. Hindawi Publishing Corporation
Case Reports in Dentistry Volume 2015, Article ID 320830,http://dx.doi.org/10.1155/2015/320830.
NANCY W. BURKHART, BSDH, EdD, is an adjunct associate professor in the department of periodontics/stomatology, Baylor College of Dentistry and the Texas A & M Health Science Center, Dallas. Dr. Burkhart is founder and cohost of the International Oral Lichen Planus Support Group (http://bcdwp.web.tamhsc.edu/iolpdallas/) and coauthor of General and Oral Pathology for the Dental Hygienist. She was a 2006 Crest/ADHA award winner. She is a 2012 Mentor of Distinction through Philips Oral Healthcare and PennWell Corp. Her website for seminars on mucosal diseases, oral cancer, and oral pathology topics is www.nancywburkhart.com. She can be contacted at [email protected].