3 hidden benefits of clear aligner therapy relating to airway health
Lauren Gueits, BS, RDH
Ben Miraglia, DDS
Clear aligners are becoming increasingly popular. Are you aware that by offering clear aligner therapy (CAT), you may also help patients breathe, sleep, and thrive? Obstructive sleep apnea (OSA) is a common disorder.1 According to the American Sleep Apnea Association, an estimated 22 million Americans are suffering from OSA, with two-thirds of the moderate to severe cases remaining undiagnosed.2 Recently, dentists have been called upon by the ADA as the “only health professionals” with the experience to prescribe oral appliance therapy.3 The question is, should CAT be considered an oral appliance to combat sleep-disordered breathing (SDB)? This article will review the three essential hidden benefits of CAT that may help patients breathe better while also giving them a beautiful smile:
1. Changing the morphology of the arch form and width
2. Increasing oral cavity volume
3. Proper tongue placement
Changing morphology of arch form and width
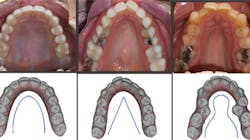
If we take the time to disclose the cause of disease, we can then focus on proper treatment modalities. The root cause of most crowded malocclusions is a result of three conditions: improper arch form, improper arch width, and improper buccolingual inclination (figure 1).
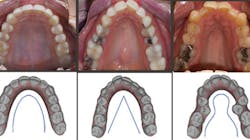
Figure 1: Examples of a proper U-shaped arch (left), an improper V-shaped arch (middle), an improper omega-shaped arch (right). Photos courtesy of Dr. Ben Miraglia.
Orthodontist James McNamara, DDS, has provided the transverse measurement, which is the shortest distance between teeth Nos. 3 and 14 at the gumline. A healthy, uncrowded width falls in the range of 35 mm to 39 mm.4 Lesser measurements will result in crowding, the most common form of malocclusion. A quick way to gauge this would be to rest a cotton roll (37 mm) in between the maxillary first molars and evaluate the fit (figure 2).

Figure 2: Measuring the transverse measurement. Photo courtesy of Dr. Ben Miraglia.
By addressing the malocclusion with CAT, we are also providing patients with a remodeled healthy arch form and width via gentle, consistent forces that promote healthy changes in the dentoalveolar complex. With consistent, low-grade pressure, as opposed to high forces and constant pressure, teeth move with the bone, not through the bone. See case examples for some remarkable results demonstrating how CAT can change arch morphology.
Having the proper arch morphology and vertical dimension leads to an increase in oral cavity volume—the second benefit of CAT.
Increasing oral cavity volume
By increasing the oral cavity volume, we are promoting nasal breathing and healthier human beings! Expanding the dentoalveolar complex not only solves crowding of the teeth, it also has the added benefit of creating more room for the tongue. Wider and more forward is a healthy direction, providing long-term solutions via increased oral cavity volume and more room for the tongue. We can compare this to retractive techniques involving extraction (EXT), distilization, and/or higher amounts of interproximal reduction (IPR)—techniques that treat the symptom instead of the cause and result in a decrease in oral cavity volume with less room for the tongue.
Many believe that IPR and EXT are necessary, but we can successfully “uncrowd” the teeth through expansion and mild proclination. This is a win-win, because most dental practitioners do not enjoy performing IPR and EXT, and patients are reluctant to receive treatment—a common barrier
Dr. Miraglia treats many patients who were seeking alternatives to retractive techniques and chose the non-EXT/minimal IPR route once educated on the benefits of expansive orthodontics versus the maladies of retractive orthodontics. Dental hygienists are key players in educating patients on the benefits of increasing oral cavity volume to help prevent and treat disease, offering patients long-term solutions. For more information on the benefits of expansive orthodontics, visit righttogrow.org.
Now that we demonstrated the cause and effect of CAT on arch morphology and increased oral capacity volume, let’s examine our third hidden benefit.
Figure 3: 36 mm is an appropriate width; the others display improper width and insufficient tongue space. Photos courtesy Dr. Ben Miraglia.

36 mm

30 mm

32 mm

25 mm
Promoting proper tongue placement
As the transverse measurement decreases, so does the “home” for the tongue. In Figure 3, you notice the narrowing of the arch and the increased vault of the palate in direct proportion to the decreasing width of the transverse (McNamara) measurement.
Conclusion
What does the research show us? You’ll see it is very compelling!
• “A narrow maxilla with [a] high arched palate characterizes a phenotype of patients with [OSA]. This is associated with increased nasal airflow resistance and posterior displacement of the tongue.”5
• “The Class II malocclusion was significantly more common in the OSA group. The V-palatal shape was a frequent finding in the OSA group.”6
• “Snoring is associated with straight profiles, V-shaped palatal morphology, increased neck circumference, decreased upper arch length, and decreased inter-first upper premolar distance.”7
• “Patients with OSA had significantly narrower maxillary and mandibular arch widths with an increase in maxillary and mandibular dental arch length when compared to control groups. These findings support the notion that a narrow maxilla or mandible may lead to airway obstruction because of inadequate space for the tongue. Thus, when the space in the oral cavity is inadequate, it is possible that a normal-sized tongue can gravitate to the back of the oro-pharynx.”8
Dr. Ben Miraglia has been successfully using CAT since 2004, essentially as an oral appliance for expansion. He explains his methodology: “I like to refer to oral cavity volume as the home for the tongue. Simply stated, good things happen when the tongue has an appropriate amount of space. Bad things happen when the tongue loses its space.” Although mandibular advancement appliances can provide short-term benefits in SDB patients, research is uncovering potential long-term effects of bite changes and exacerbation of patients’ OSA. Mandibular advancement may lead to maxillary retraction through what is known as the “head gear effect.”9,10 Having proper tongue placement, where the tongue is given the space to create a suction in the palate rather than the tongue falling down and back, is critical to avoid symptoms of SDB ranging from snoring to OSA.
CAT is already a sought-after treatment with great compliance. Meanwhile, dentists have been called upon by the ADA to diagnose and prescribe oral appliance therapy to their SDB patients. The next time a patient needs oral appliance therapy, perhaps dental practitioners will consider CAT as a viable, noninvasive first option. Now that you are aware of the three hidden benefitsCAT provides through (1) expansion, (2) increased oral cavity volume, and (3) proper tongue placement, let’s make sure patients are aware of these benefits too! It’s up to all dental practitioners to educate patients about all the options to help them breathe, sleep, and thrive.
Authors’ note:For more information on how to provide your patients with expansive orthodontic techniques, visit airwayhealthsolutions.com.
Case examples
Case 1: 27-year-old male: 2-year clear aligner treatment. There was an estimated 8 mm to 10 mm increase in the transverse measurement. Case and photos courtesy of Dr. Daniel Noor.
Case 2: 48-year-old female: 15-month clear aligner treatment. This case demonstrates an improvement in a remodeled alveolar complex and an increase in vertical dimension. Case and photos courtesy of Dr. Ben Miraglia.


Before: V-shaped arch. After: U-shaped arch.


Before: Severe deep bite. After: Improved vertical dimension.


Before: V-shaped arch. After: U-shaped arch; implant placed No. 14.
Case 3: 17-year-old male: 1-year treatment. Expanding and proclining delivered more room for the tongue and increased oral cavity volume without IPR or extractions. Case and photos courtesy of Dr. Ben Miraglia.




Before: V- and omega-shaped arch, crossbite. After: U-shaped arch, no IPR, no EXT, increased oral cavity volume.
References
1. Franklin KA, Lindberg E. Obstructive sleep apnea is a common disorder in the population-a review on the epidemiology of sleep apnea. J Thorac Dis. 2015;7(8):1311-1322. doi:10.3978/j.issn.2072-1439.2015.06.11.
2. Sleep Apnea Information for Clinicians. American Sleep Apnea Association website. https://www.sleepapnea.org/learn/sleep-apnea-information-clinicians/.
3. ADA adopts policy on dentistry’s role in treating obstructive sleep apnea, similar disorders [news release]. Chicago, IL: American Dental Association Media Relations; October 23, 2017. https://www.ada.org/en/press-room/news-releases/2017-archives/october/ada-adopts-policy-on-dentistry-role-in-treating-obstructive-sleep-apnea.
4. McNamara JA. Maxillary transverse deficiency. Am J Orthod Dentofac Orthop. 2000;117(5):567-570. http://www.dent.umich.edu/sites/default/files/departments/opd/160.pdf.
5. Johal A, Conaghan C. Maxillary morphology in obstructive sleep apnea: a cephalometric and model study. Angle Orthod. 2004;74(5):648-656.
6. Banabilh SM, Samsudin AR, Suzina AH, Dinsuhaimi S. Facial profile shape, malocclusion and palatal morphology in Malay Obstructive Sleep Apnea Patients. Angle Orthod. 2010;80(1):37-42.
7. Al-Madani GH, Banabihl SM, El-Sakhawy MM. Prevalence of snoring and facial profile type, malocclusion class and dental arch morphology among snorer and nonsnorer university population. J Orthodont Sci. 2015;4(4):108-12.
8. Banabilh SM, Suzina AH, Dinsuhaimi S, Samsudin AR, Singh GD. Dental arch morphology in south-east Asian adults with obstructive sleep apnea: geometric morphometrics. J Oral Rehabil. 2009;36(3):184-92. doi:10.1111/j.1365-2842.2008.01915.x.
9. Marklund M. Long-term efficacy of an oral appliance in early treated patients with obstructive sleep apnea. Sleep Breath. 2016;20(2):689-94. doi:10.1007/s11325-015-1280-1.
10. The story of headgear. Right to Grow website. https://www.righttogrow.org/.
Lauren Gueits, BS, RDH, is founder and president of Lauren Gueits & Associates, a clinician of more than 30 years, and a recipient of the 2010 RDH Sunstar Award of Distinction. She lectures nationally on airway health solutions, comprehensive care, and oral-systemic links. She received her degree from the State University of New York at Farmingdale in 1991 and postgraduate training through the Academy of Myofunctional Therapy in 2013.
Ben Miraglia, DDS, has been providing expansive orthodontics and functional appliance therapy for more than 15 years. He has been voted one of the top educators of the year by Dentistry Today and was honored with a position on the President’s Council of Northern Westchester Hospital. Dr. Miraglia is on the American Academy of Cosmetic Orthodontics Board of Directors and the American Academy of Physiological Medicine and Dentistry.