Oral pathology is not about naming lesions; it’s about learning how to see
Key Highlights
- Accurate oral pathology begins with intentional observation—not speed, intuition, or premature interpretation—making visual assessment a trained clinical skill.
- Dental hygienists play a critical role in early recognition through careful observation, precise documentation, and continuity of care, even though diagnosis remains the dentist’s responsibility.
- Separating observation from interpretation improves lesion evaluation, strengthens interdisciplinary communication, and enhances patient safety, especially in complex and medically diverse populations.

During a routine intraoral examination, it is easy to fall into the familiar phrase, “Everything looks fine.” We move quickly, following a sequence we have repeated hundreds of times, confident in our efficiency. But oral pathology does not begin with efficiency; it begins with observation. And observation, unlike we were often taught, is not automatic.
Some oral disorders present with signs and symptoms that appear pathognomonic for a specific condition, while others present with remarkably similar clinical features that make accurate recognition challenging.1 Because of this, even when a lesion seems to “fit the picture,” careful observation remains absolutely nonnegotiable. Ultimately, being clinically confident is not built on recognition alone, but on the ability to observe, connect findings, and place them within the full patient context.2
In dental education, oral pathology is frequently presented as a catalog of lesions to memorize—names, colors, locations, associations, and so on. While this knowledge is essential, it often overshadows a more fundamental skill: learning how to truly see. Because before we learn how to name lesions, we must first learn how to observe them.3
For dental hygienists, this distinction matters deeply. We are often the first professionals to evaluate oral tissues consistently over time. Our ability to observe, without rushing to interpret, can influence early recognition, documentation quality, interdisciplinary communication, and ultimately, patient safety.
Observation is not intuition
Many clinicians describe their clinical judgment as intuition. “I just know when something doesn’t look right.” And while experience certainly sharpens perception, observation is not intuition; it is a trained skill. True clinical observation is deliberate; it requires attention, structure, and the willingness to pause. Intuition may alert us that something feels off, but observation is what allows us to describe why.
Without structured observation, clinicians rely on mental shortcuts—pattern recognition without analysis, assumptions based on familiarity, or premature conclusions.4 These shortcuts may feel efficient, but they increase the risk of oversight, especially when lesions present subtly or evolve slowly.
Observation is not about being slow; it is about being intentional. It is the foundation upon which sound clinical reasoning is built.
What we miss when we skip the foundations
When observation skills are underdeveloped, the consequences are not always dramatic, but they are significant. Documentation becomes vague, lesions are described imprecisely or not at all, subtle changes over time go unnoticed, referrals tend to lack clarity, and, in some cases, early signs of pathology are simply missed.
Dental hygienists play a critical role as continuity-of-care providers. We often see patients more frequently than other clinicians, placing us in a unique position to detect changes in oral tissues. But this role can only be fulfilled when observation is treated as a professional responsibility—not a passive step before diagnosis.
It is important to clarify a critical distinction: observation is not diagnosis. Dental hygienists are not expected to label lesions or establish definitive diagnoses. Our role, however, is essential. Through careful and consistent observation, hygienists are often the first to recognize subtle changes in oral tissues, changes that may otherwise go unnoticed.5 When paired with precise documentation, this observational role becomes the foundation for timely evaluation, effective interdisciplinary communication, and patient-centered care.6 Observation does not replace diagnosis, but it initiates and supports the clinical process that leads to it.
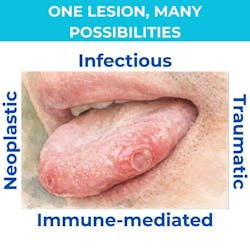
One lesion, many possibilities: Understanding clinical spectrums
A single clinical presentation may represent a wide spectrum of underlying conditions. Ulceration, for example, is a commonly presenting sign in the oral cavity and may be associated with numerous etiologic factors. Clinically similar ulcerated lesions can arise from infectious, immune-mediated, traumatic, or neoplastic processes (figure 1). Overlap in clinical and even histologic features often makes these lesions particularly challenging to evaluate.
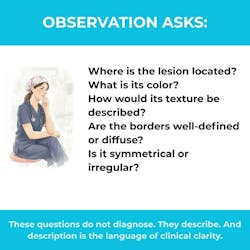
This is precisely why observation must precede interpretation. Without a structured visual assessment—location, borders, surface characteristics, chronicity, and associated symptoms—the clinician risks narrowing the differential diagnosis too early (figure 2).
Oral pathology often requires a detective mindset: gathering clues, connecting patterns, and resisting the urge to label prematurely. This approach not only improves clinical accuracy but also strengthens how findings are communicated to the dental team, specialists, and, critically, to the patient.
Clear observation allows us to explain what we are seeing, what we are monitoring, and what the next steps may be, helping to reduce patient anxiety in the presence of oral alterations.
Seeing before interpreting: A clinical shift
One of the most common pitfalls in oral pathology education is the urge to interpret too early. The moment a lesion is seen, the mind jumps to possibilities: Is it frictional keratosis? Leukoplakia? Lichen planus?
This cognitive leap is understandable, but risky.
Interpretation without adequate observation limits accuracy. It narrows perception and biases what we notice next. Instead of fully assessing the lesion, we unconsciously search for features that confirm our initial assumption.7
A more effective approach is to separate observation from interpretation.
Training the eye: A skill, not a talent
The clinical eye is often described as a natural talent—something you either have or develop by chance over time. In reality, visual diagnostic skills can be trained intentionally.
Repetition alone is not enough. Exposure without structure does not guarantee improvement. What sharpens observation is guided visual learning: comparing normal variations, recognizing surface patterns, understanding how pathology evolves visually, and learning restraint in interpretation.8
Before clinicians can confidently recognize disease, they must be deeply familiar with normal, and the many ways normal can vary. Only then can deviations be identified with accuracy.
Why this matters more than ever
The clinical recognition and evaluation of oral mucosal lesions play a critical role in the early detection of oral cancer and potentially malignant disorders. Literature consistently emphasizes that most oral cancers and premalignant lesions are clinically detectable in their early stages when careful examination is performed. The World Health Organization recommends that any suspicious oral lesion that does not resolve within approximately two weeks after removal of local irritants should be further investigated, often through biopsy.⁹
While the detection of malignancy remains a priority, it is equally important to recognize that benign and inflammatory lesions can significantly impact patients’ comfort, function, and quality of life. Pain, burning, ulceration, and chronic mucosal changes deserve the same level of observational precision and professional attention.
Modern dental patients present with complex medical histories, polypharmacy, esthetic treatments, and chronic systemic conditions, all of which may influence oral tissues in subtle ways. In this context, strong observational skills are not optional; they are essential.
Seeing is a professional responsibility
Returning to that routine intraoral exam, the difference is not time—it is intention. Observation transforms a checklist into a clinical encounter. It replaces assumptions with awareness.
Oral pathology is not about naming lesions; it is about learning how to see what is in front of us, describing it with intention, and understanding its potential significance over time.
For dental hygienists, observation is not optional, nor is it intuitive. It is a skill to be trained, refined, and honored. Because the better we see, the better we serve, and the safer our patients become.
Who should evaluate? Shared responsibility in oral lesion screening
In many dental practices, soft-tissue evaluations and oral cancer screenings are routinely performed by dental hygienists. This is not incidental. Hygienists are often the clinicians who spend the most consistent and uninterrupted time examining oral tissues over the course of a patient’s care. Most are well trained in visual screening techniques and feel confident in their ability to identify abnormal findings. However, this clinical reality carries weight.
Delegation of oral mucosal screening, whether formal or informal, does not transfer diagnostic responsibility. While dental hygienists play a critical role in observing, documenting, and communicating clinical findings, the responsibility for diagnosis, confirmation, and follow-up ultimately remains with the dentist. This distinction extends beyond professional boundaries; it carries ethical and legal implications that protect both the patient and the integrity of care.
Many dental hygienists describe a recurring concern when abnormalities they have carefully documented are not fully evaluated or acknowledged. When observations are overlooked or not followed by a confirmatory examination, continuity of care is disrupted. In these moments, the issue is not one of authority, but of missed opportunity, and patient safety may be compromised.
For this reason, clearly defined roles and respectful clinical communication are essential. Observation must be recognized as meaningful clinical input, documentation must be precise and actionable, and referrals or follow-up examinations must occur in a timely manner. In most jurisdictions, diagnostic responsibility cannot be delegated by law, and delegation does not relieve the dentist of accountability.
When professional roles are clearly understood and consistently upheld, the clinical process becomes safer, more effective, and genuinely collaborative. This dynamic underscores why the quality of observation matters so deeply. Precise, descriptive documentation does more than record findings; it empowers the dental team, supports meaningful interdisciplinary dialogue, and ensures that concerns identified during hygiene appointments are translated into appropriate clinical action.
Oral pathology is not managed in isolation. It is navigated through collaboration, where dental hygienists observe and communicate with clarity, and dentists evaluate, diagnose, and guide treatment responsibly. When each role is respected and exercised with intention, patient care is not only strengthened, but elevated.
Editor's note: This article appeared in the March 2026 print edition of RDH magazine. Dental hygienists in North America are eligible for a complimentary print subscription. Sign up here.
References
- Epstein JB, Zhang L, Rosin M. Advances in the diagnosis of oral premalignant and malignant lesions. J Can Dent Assoc. 2002;68(10):617-621.
- Islam NM, Alramadhan SA. Lichenoid lesions of the oral mucosa. Oral Maxillofac Surg Clin North Am. 2023;35(2):189-202. doi:10.1016/j.coms.2022.10.005
- Sucre A. The importance of properly recording oral pathologies for dental hygienists. RDH. October 30, 2024. https://www.rdhmag.com/pathology/oral-pathology/article/55239158/the-importance-of-properly-recording-oral-pathologies-for-dental-hygienists
- do Carmo MA, Gleber-Netto FO, Romano ML, Caldeira PC, de Aguiar MC. Clinical and demographic overlaps among immunologically mediated oral diseases: a challenge for clinicians. Gen Dent. 2014;62(1):67-72.
- Alexander RE, Wright JM, Thiebaud S. Evaluating, documenting and following up oral pathological conditions. A suggested protocol. J Am Dent Assoc. 2001;132(3):329-335. doi:10.14219/jada.archive.2001.0175
- Teusner DN, Amarasena N, Satur J, Chrisopoulos S, Brennan DS. Applied scope of practice of oral health therapists, dental hygienists and dental therapists. Aust Dent J. 2016;61(3):342-349. doi:10.1111/adj.12381
- Brocklehurst P, Pemberton MN, Macey R, Cotton C, Walsh T, Lewis M. Comparative accuracy of different members of the dental team in detecting malignant and non-malignant oral lesions. Br Dent J. 2015;218(9):525-529. doi:10.1038/sj.bdj.2015.344
- Sbricoli L, Zago R, Cavallin F, Stellini E, Bacci C. Diagnostic ability in oral pathology among different population clusters. Oral Dis. 2024;30(4):2278-2284. doi:10.1111/odi.14689
- Warnakulasuriya S, Kujan O, Aguirre-Urizar JM, et al. Oral potentially malignant disorders: a consensus report from an international seminar on nomenclature and classification, convened by the WHO Collaborating Centre for Oral Cancer. Oral Dis. 2021;27(8):1862-1880. doi:10.1111/odi.13704
About the Author

Andreina Sucre, MSc, RDH
Andreina Sucre, MSc, RDH, is an international dentist, oral pathology, and oral surgery specialist practicing dental hygiene in Miami, Florida. A passionate advocate for early pathological diagnosis, she empowers colleagues through lectures focused on oral pathologies. Andreina is the founder of The Patho RDH, a published author for RDH magazine, and a selected speaker at RDH Under One Roof 2026. Committed to community outreach, she educates non-native English-speaking children on oral health and actively volunteers in dental initiatives.