Soft tissue therapy with lasers
Hygiene department in general practice incorporates lasers as nonsurgical option.
Nora Raffetto, RDH, and
Teri Gutierrez, RDH
With the advent of the Nd:YAG fiber optical systems, laser technology is becoming widely available for soft tissue management programs within the general practice setting. Having used lasers since 1993 in our general practice settings, this article is a retrospective compilation of cases.
The approximate number of patients treated was 800. The sample size used for the study was 110 patients. Results of the study have led to the development of a laser soft tissue management program for the general practice setting.
The purpose of a continual soft tissue management program is to restore and maintain the periodontal tissues so that there is:
- elimination of the diseased sulcular epithelium
- minimal intrasulcular bacterial activity
- a halting of the apical migration of the epithelial attachment
- minimal pocket depth
- no bleeding on probing
The most effective diagnostic procedure for periodontal disease is the periodontal probe technique. To be complete, each periodontal probing should include, per tooth: six-point measurement; bleeding sites; recession; furcations; mobility; and exudate. For consistency, a Marquis-type probe was used for all probing in the study.
Once the probing has been done, the doctor and the hygienist can make a definitive diagnosis of the presence of periodontal disease, as well as the current stage of the disease. These stages of disease are referred to as case types. Case types are determined according to the pocket depths, as well as the presence of any other disease indicators. Case types range as follows:
- Healthy
- Type I - gingivitis
- Type II - beginning periodontitis (3 mm and 4 mm)
- Type II-III - moderate periodontitis (4 mm and 5 mm)
- Type III+ - advanced periodontitis (5 mm and 6 mm)
- Type IV+ - severe periodontitis (6-plus mm)
The study was limited to case types I-III, which are very manageable within the general practice setting.
Treatment planning is the key to successful soft tissue management with lasers. The completion of probing will aid the doctor and hygienist in selecting the number of hours of treatment. The following is a recommendation as to how many hours of treatment are needed for the various case types:
> Healthy, one appointment
> Gingivitis (Type I), two to three hours
> Beginning periodontitis (Type II), two to four hours
> Moderate periodontitis (Type III), four to six hours
> Advanced periodontitis (Type IV), six to 10 hours
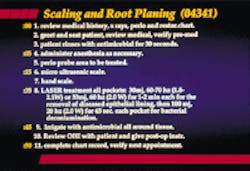
At typical appointments, each hour of laser soft tissue therapy consisted of the following protocol (see Figure 1):
- Anesthesia as needed: injection, dyclone, or benzocaine 20 percent
- Ultrasonic scaler with antimicrobial irrigant (chlorhexidine was used as the antimicrobial irrigant in the study)
- Light hand instrumentation as needed
- Laser removal of diseased epithelial lining
- Laser bacterial decontamination
- Ultrasonic antimicrobial irrigant
- Postoperative instructions and home care instructions
Treatment begins in the most diseased site presented and proceeds progressively to the least diseased sites. At each therapy appointment, any previously treated sites should be treated again. This involves repeating steps of bacterial decontamination with a laser and irrigation with an antimicrobial. It must be pointed out that when treating a site again during a subsequent appointment, care should be taken to decrease the depth of fiber and ultrasonic tip insertion, as early healing and attachment should not be disturbed. A timeline for one hour of soft tissue therapy with lasers can be found in accompanying chart.
Laser techniques
The two techniques used during soft tissue therapy with lasers are de-epithelialization and bacterial decontamination. Each technique requires different laser parameters, as well as different hand movements. Laser parameters used in this study can be seen in related charts (Figures 2 and 3). The authors have no financial interest in any laser company, but, for the sake of clarity, the laser used in this study was American Dental Technologies` Pulsemaster.
Laser de-epithelialization, or laser curettage, begins at the crest of the gingival margin and progresses to the base of the pocket. The fiber tip should be measured out according to the depth of the site being treated. The fiber is placed in contact with the gingiva. The tip is angled toward the tissue wall and away from the tooth surface. A sweeping motion both vertically and horizontally - not unlike the cross-hatch technique in root planing - is done to the base of the pocket. Lasing is complete when a fresh bleed is present.
On the other hand, laser bacterial decontamination is done at the end of the therapy session. The tip of the fiber should be cleaved in order to have full power delivered from the fiber tip into the tissues. Keeping the fiber tip in contact with the tissue and constantly moving, the tissue wall should be lased for 30 seconds to one minute.
After decontamination, the site is flushed with antimicrobial irrigant by using the ultrasonic scaler.
Two cases
In one case, sulcular debridement with a laser was an adjunctive treatment of moderate periodontal disease. The case demonstrates the effectiveness of using the pulsed Nd:YAG PulseMasterJ laser in conjunction with scaling and root planing (using microultrasonic instrumentation) in treating mild-to-moderate periodontitis. Dr. Donald Coluzzi diagnosed the case and planned the treatment sequence. Therapy was provided by one of the authors under the direct supervision of Dr. Coluzzi in compliance with California`s dental practice act.
During pretreatment, five diagnostic tests were run. The clinical examination was done on a 56-year-old female. The tooth vitality was all within normal limits, and hard tissue tests showed broken-down dentition. The radiographic exams revealed moderate and generalized horizontal bone loss, as well as recurrent caries around restorations. Tests on the soft tissue displayed inflammation, calculus, 5-6 mm pockets, and bleeding on probing (see Figure 4).
The diagnosis was Type III moderate periodontitis. Treatment involved scaling and root planing using microultrasonics and sulcular debridement. Possible treatment alternatives included surgery with no laser instrumentation. The indications were inflammatory tissue and diseased epithelial lining of the pockets.
The treatment objective was to restore periodontal health via laser operating parameters of 30mJ, 60Hz, 1.8W, 30 to 60 seconds per pocket, followed by microultrasonic instrumentation, then 100mJ, 20Hz, 2.0W, 30 to 60 seconds per pocket. The treatment sequence was weekly appointments of one-hour duration for a total of six hours. The laser was used for 10 minutes during the one-hour appointment.
The laser fiber was calibrated for the pocket depth and was placed at the top of the sulcus. The fiber was held parallel to the root surface, but always kept on the diseased tissue. The fiber was moved both horizontally and vertically. Diseased tissue was removed by withdrawing the fiber. No complications were experienced. The diseased epithelial tissue was easily removed with excellent hemostasis. Patient management was excellent with topical anesthesia only.
The prognosis was good if compliance with home care instructions was heeded. Follow-up care showed no side effects or complications. Pocket reduction resulted, and the tissue tone returned. The healing assessment showed the pocket depths had decreased markedly with no inflammation (see Figure 5).
The follow-up appointments were done at one and three months. The one-month postoperative appointment is used for patient monitoring of healing and home care. No probing is done at this appointment. However, retreatment with the laser for bacterial decontamination is performed at sites still demonstrating inflammation.
At the three-month appointment for supportive periodontal therapy, probing determines the improvement in pocket depth from soft tissue therapy with the laser. In this case, most pocket reductions fell into the 1 mm to 3 mm range, and some sites showed as much as 4 mm of improvement. Tissue tone, color, stippling, and texture also showed improvement.
In another case, soft tissue therapy was combined with conventional osseous surgery. The purpose of the case was to restore existing severe periodontal lesion with a laser, which was followed by a bone graft surgery.
The patient was a 40-year-old male who had a positive medical history for high blood pressure, diabetes, and allergies. He was being medicated with chlorine for gout. The clinical exams revealed extremely broken-down dentition, as well as Type IV, severe periodontitis. The periodontal probing indicated a 12 mm infrabony defect on the mesial-facial of #6 (see Figure 6).
Dr. Robert Barr diagnosed and planned treatment for the case. One of the authors provided the therapy under direct supervision in compliance with the dental practice act in California. The treatment plan called for scaling and root planing with laser curettage, which would be followed by bone graft surgery.
In order to treat the entire oral cavity, the patient received 10 hours of laser therapy for the soft tissue. The first full hour was devoted to tooth #6. After microultrasonics and scaling with light root planing, the laser curettage was set to the following parameters with a Pulsed Nd:YAG: 1064 nm - 300 micron fiber; 30mJ, 60Hz, 1.8W. Each site was treated for 40 to 60 seconds and followed by microultrasonics.
The parameters for the bacterial decontamination were: 100mJ, 20Hz, 2.0W. Each site was treated for 30 seconds, followed by the delivery of antimicrobial irrigant with microultrasonics.
The first hour of therapy was devoted to tooth #6 (see Figure 7). During subsequent weekly appointments, the tooth was treated again following the decontamination parameters. A local anesthetic was used at the site during the first four appointments. After each treatment with the laser, the site was irrigated with the antimicrobial agent. The laser fiber and ultrasonic tip were measured shorter at each "re-treat" so that new attachment was not disturbed.
The patient also was seen at one- and three-month periodontal therapy appointments. The one-month appointment involved a visual assessment of healing and retreatment of any sites showing residual inflammation. Pocket reduction was determined at the three-month appointment. At each evaluation, the patient reported no adverse effects from the therapy. Long-term care was advised in order to monitor patient compliance with the critically important home care.
The probing at the three-month appointment revealed a 3 mm reduction in pocket depth along with a return of color, texture, stippling, and no bleeding. Indeed, there was blanching on probing even with a 9 mm defect. It was determined that the patient would be placed into periodontal maintenance (two-month recall) with an evaluation for the bone graft surgery after six months.
At the six-month evaluation, the doctor determined that the site was ready to receive a bone graft. Surgery was done in the office under local anesthetic. The site was flapped open and examined for residual debris. The doctor then placed freeze-dried, demineralized ground cortical bone into the site.
The flap was sutured closed, and the patient was given postoperative instructions. The sutures were removed after one week, along with a visual exam. The patient was appointed for evaluation of the tissue in one and three months.
The probing at the three-month appointment revealed a healthy 3 mm pocket with improved color, texture, stippling, blanching, and no bleeding (see Figure 8).
Soft tissue therapy with lasers has proven to be a viable, nonsurgical alternative therapy in the treatment of periodontal disease. Patients respond favorably to treatment with minimal post-operative discomfort, and some patients reported no discomfort at all. The laser, as an instrument in the dental operatory, does have a learning curve that most practitioners claim is mastered quickly. With proper training and certification, the laser is a safe, effective, and highly selective instrument that can be used effectively within the general practice setting.
Nora Raffetto, RDH, graduated in 1971 from Cabrillo College and has been practicing in a general practice setting for more than 24 years. She holds a Category III Hygiene Mastership certificate from the Academy of Laser Dentistry, is a member of the certification committee, is the dental hygiene representative on the Academy board and has presented to and trained dentists and dental hygienists throughout the United States in laser soft tissue management.
Teri Gutierrez, RDH, graduated from Foothill College in 1990 and has been practicing in the general practice setting for nine years. Having attained a Category III Hygiene Mastership from the Academy of Laser Dentistry, Ms. Gutierrez serves as an examiner for the Academy during certification at both local certification sites and the annual conference. Ms. Gutierrez also provides hands-on laser soft tissue training through her consulting business, Soft Tissue Laser Training.
References
* White JM, Goodis HE, Rose CL. Use of the pulsed Nd:YAG laser for intraoral soft tissue surgery. Lasers Surg Med. 1991;11(5):455-461.
* White JM, Goodis HE, Chavez EM, et al. Photothermal laser effects on intraoral soft tissue in vitro. J Dent Res. 1992;71:221 (Abstract #925).
* Meserendino LJ, Pick RM. Lasers in dentistry. Quintessence Books, 1995.
* Neil ME, Mellonig JT. Clinical efficacy of the Nd:YAG laser for combination periodontitis therapy. Pract Perio Aesthst Dent. 1997;9(6):1-5 (supplement).
* Lin PP, Beck FM, Matsue M, et al. The effect of a pulsed Nd:YAG laser on periodontal pockets following subgingival application. J Dent Res. 1992;71:299 (Abstract #1548).
* Dental Practice Act, State of California, section 1088,d,2.
* Department of Health and Human Services. K961269, March 10,1997.
* O?Grady and Williams. Advanced Hygiene Concepts.
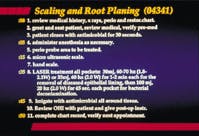
Figure 1 A timeline for our hour of soft tissue therapy with a laser.
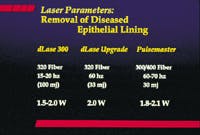
Figure 2 Parameters for laser curettage.
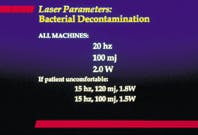
Figure 3 Parameters for bacterial decontamination with a laser.
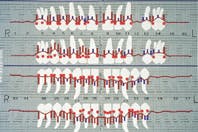
Figure 4 Results of periodontal charting at clinical exam for 56-year-old female.

Figure 5 Results of periodontal charting after laser therapy.
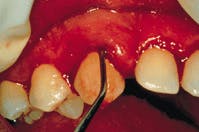
Figure 6 A 12mm infrabony defect was noted on the mesial-facial of tooth #6.

Figure 7 Laser curettage is performed on tooth #6.

Figure 8 Probing after laser treatment and osseous surgery reveals healthy 3mm pocket.