Antioxidants, free radicals, and oxidative stress
by Karen Davis, RDH, BSDH
[email protected]
What does oxidative stress have to do with oral-systemic health? The answer to this question is a topic that has many layers to it, and the data surrounding this topic is an area of current explosion in medical and dental literature. My guess is that many colleagues and dental team members are somewhat foggy on the topic, but the reason it is important to grasp this is because — as the science surrounding chronic inflammation continues to unfold — oxidative stress appears to be a player in the cascade of events that link oral and systemic health. Antioxidants themselves could be helpful in interrupting that cascade.
A logical place to begin is with explanations that may remind you of your physics class, but I challenge you to take a moment to digest this as it helps in understanding the oral/systemic connection. The body is made up of many types of molecules, atoms, and cells. Atoms within the body are considered to be stable when every electron in the outermost shell has a complementary electron that spins in the opposite direction.
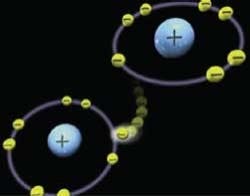
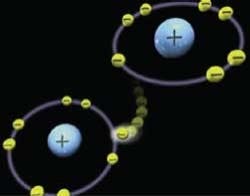
Free radicals involving oxygen or reactive oxygen species (ROS) refer to atoms with at least one unpaired electron in the outermost shell, and as a result are unstable or reactive. To become stable, they must obtain or “steal” an electron from another molecule, which can begin a chain reaction of “electron stealing,” and the production of more free radicals as shown in Figure 1. Antioxidants can also contribute an electron to a free radical, thereby stabilizing the molecule. While some free radicals occur naturally, and some are produced by the body’s immune system to help neutralize viruses and bacteria, it is the excess of free radicals that becomes dangerous to our health.
Oxidative stress refers to the imbalance of too many free radical molecules and can lead to damage of the cell membrane, DNA, protein, and fats. It is this cellular damage which, in turn, can lead to the aging process and degenerative diseases such as cardiovascular diseases, aging, immune dysfunction, Alzheimer’s disease, diabetes, and even cancer.
In the case of diabetes and its subsequent impact on the development of cardiovascular disease, there is growing evidence that excess generation of highly reactive free radicals (largely due to hyperglycemia), causes oxidative stress, which is a major risk factor for the development of heart-muscle disease referred to as cardiomyopathy.1 Studies have also implicated oxidative stress and decreased antioxidant capacity to the development of oral squamous cell carcinoma.2,3
The oral environment is especially susceptible to damage from free radicals because the mucous membrane allows for rapid absorption of various substances, which contribute to oxidative stress such as hydrogen peroxide in whitening products, alcohol, nicotine, and even some dental materials used in restorations. Periodontal infection can also contribute to the development of oxidative stress, and oxidative stress in and of itself can exacerbate inflammation both in the oral cavity and systemically.
A recent study published in the Journal of Dental Research titled, “Oxidative Stress, Systemic Inflammation, and Severe Periodontitis,” set out to examine the association between oxidative stress and systemic inflammation in people with severe periodontitis.4 They compared measurements of oxidative stress and blood antioxidant potential and measured C-reactive protein, interleukin-6, total HDL, LDL cholesterol, and triglyceride levels on individuals with severe generalized periodontitis and compared measurements against control individuals with no history or clinical signs of periodontitis. Results revealed that individuals with severe periodontitis exhibited higher oxidative stress levels, and lower total antioxidant capacity compared to healthy individuals — independent of age, gender, smoking habits, ethnicity, and standard differences in the overall lipid panel. Oxidative stress levels were positively correlated with levels of CRP and clinical periodontal parameters. The authors concluded “that severe periodontitis is independently associated with increased oxidative stress and reduced antioxidant capacity.”
Researchers Chapple and Matthews published a comprehensive review of free radicals and antioxidants in periodontal destruction and their data suggests that oxidative stress lies at the heart of periodontal tissue damage that results from host-microbial interactions.5 The cascade of events that results in tissue damage is either directly involved as the result of excess ROS activity and antioxidant deficiency; or indirectly involved as a result of creating a pro-inflammatory state.
Incorporating antioxidants into therapy
It is the researchers’ conclusion that improved understanding in these pathways provides opportunities for the development of novel antioxidant therapies, which could function not only as antioxidants but also as anti-inflammatory agents.
To that point, dental professionals should be aware of a line of products by PerioSciences which provide antioxidants for topical application, and immediate absorption into the oral tissues, which can help to offset oxidative stress, thereby improving conditions such as lichen planus, xerostomia due to chemotherapy, geographic tongue, and many other tissue irritations. AO ProVantage and AO ProVantage Blast are antioxidant gels that contain ferulic acid, a polyphenol found in seeds and leaves of plants, and phloretin, a flavonoid derived from apples, strawberries, and tomatoes, along with thymol, essential oils, and xylitol.
The mouthwash from PerioSciences includes the antioxidants ferulic acid, curcuminoids, and green tea catechin along with essential oils. An interesting study published in the November 2010 Journal of Periodontology investigated the effects of ferulic acid and phloretin on cells impregnated with nicotine and found that concentrations of these antioxidants literally helped to counteract many of the deleterious effects of nicotine when added to the cells.6 More information about their line of products is available at www.PerioSciences.com.
Dietary methods for increasing antioxidant capacity include significant increases in antioxidant-rich foods such as pomegranates, strawberries, blueberries, raspberries, walnuts, sunflower seeds, ginger, and bright colored vegetables. Sustaining a diet rich in antioxidants every day is somewhat unrealistic for many individuals. Therefore, the addition of antioxidant supplements that have been shown to have high bioavailability for absorption, such as Juice Plus or Life Pak Nano by Pharmanex, should be considered as an adjunct for patients with periodontal disease, or for those wishing to prevent it.
As I have mentioned in previous columns, seemingly exhaustive information is available from www.dentalantioxidants.com on the topics of oxidative stress and antioxidants. As the interaction between oral and systemic health becomes even clearer, it is apparent that intercepting and treating periodontal infections, and decreasing oxidative stress in the oral environment have the potential for reducing the overall burden of oxidative stress systemically. That should be considered a win-win for oral and systemic health!
References
1. Thandavarayan RA, Diridharan VV, Watanabe K, Konishi T. Diabetic cardiomyopathy and oxidative stress: role of antioxidants. Cardiovasc Hematol Agents Med Chem 2011; Sept . 9 [Epub ahead of print].
2. Korde SD, Basak A, Chaudhary M, Goyal M, Vagga A. Enhanced nitrosative and oxidative stress with decreased total antioxidant capacity in patients with oral precancer and oral squamous cell carcinoma. Oncology 2011;80:382-389.
3. Patel JB, Shah FD, Shukla SN, Shah PM, Patel PS. Role of nitric oxide and antioxidant enzymes in the pathogenesis of oral cancer. J Cancer Res Ther 2009;5:247-253.
4. D’Aiuto F, Nibali L, Parkar M, Patel K, Suvan J, Donos N. Oxidative stress, systemic inflammation and severe periodontitis. J Dent Res 2010;89:1241-1246.
5. Chapple ILC, Matthews JB. The role of reactive oxygen and antioxidant species in periodontal tissue destruction. Periodontol 2000 2007;43:160-232.
6. San Miguel SM, Opperman LA, Allen EP, Zielinski J, Svoboda KH. Antioxidants counteract nicotine and promote migration via RacGTP in oral fibroblast cells. J Periodontol 2010: 81:1675-1690.
Antioxidants, free radicals, and oxidative stress
Karen Davis, RDH, BSDH, is the founder of Cutting Edge Concepts, an international continuing education company, and practices dental hygiene in Dallas, Texas. She is an independent consultant to the Philips Corp. and serves on the review board for Dentalantioxidants.com. She can be reached at [email protected].
PerioTeam Take-aways
1. Identify various sources of oxidative stress in the oral environment such as tobacco, alcohol, periodontal diseases, and hydrogen peroxide
2. Engage patients in conversations about how increased antioxidants can offset the impact of oxidative stress 3. Introduce patients to products such as the PerioSciences antioxidant gels and mouthwash to help offset oxidative stress.
Past RDH Issues