The efficacy and benefits of fluoride varnish with CPP-ACP

Introduction
According to the Centers for Disease Control and Prevention (CDC), “one in five people have untreated tooth decay” (see infographic).1 Two or more applications of fluoride varnish per year can prevent cavities in adults and reduce almost 40% of caries in children with primary dentition.1 The use of topical fluorides helps to remineralize enamel as well as inhibit bacterial metabolism, thus minimizing plaque bacterial growth. Topical fluoride can be given as a paste, gel, foam, rinse, or varnish. However, due to a lack of clinical evidence on the efficacy of one-minute fluoride foam or gel treatments, the only fluoride treatments currently recommended are four-minute fluoride treatments or fluoride varnish.
The benefits of CPP-ACP

Casein phosphopeptides (CPP), naturally found in milk, bind to oral surfaces and enhance enamel acid resistance while also increasing salivary fluoride levels.3 Amorphous calcium phosphate (ACP) is a reactive and soluble calcium phosphate compound that rapidly remineralizes enamel and dentin. When it forms on tooth enamel and within the dentin and dentinal tubules, it creates a reservoir of remineralizing ions within the saliva. This helps with fluoride uptake and strengthens teeth.4 When dentinal tubules are filled with ACP, the ACP converts to tooth mineral. At the same time ACP is remineralizing the tooth, it is also increasing fluoride efficacy and decreasing hypersensitivity by obstructing dentinal tubules.5
MI Varnish became available in 2012, but third-party research into the development of Recaldent began in the 1980s.6 Reynolds and colleagues at Melbourne Dental School at the University of Melbourne researched casein protein in milk.⁷ They were able to isolate the CPP-ACP complex from casein protein and identify its preventive properties, which led to the development of Recaldent. The FDA approved Recaldent in early 1999, and it has since been used to help protect teeth in products all around the world.
CPP-ACP works by binding to the surface of the tooth as well as the bacteria in plaque that is present on the tooth surface. Once in contact, a high concentration of ACP is deposited to the tooth surface. When exposed to acidic conditions, CPP-ACP acts as a buffer for free calcium and phosphate ions, significantly increasing calcium phosphate levels in plaque bacteria, thus inhibiting demineralization and enhancing the remineralization process.
CPP-ACP is an excellent adjunct for controlling dental caries in moderate- to high-risk patients, reducing decalcification and enhancing remineralization in patients undergoing orthodontic treatment, and reducing erosion in patients with reflux. Some studies have shown a significant decrease in xerostomia as a result of CPP-ACP treatment.⁷ It has been observed that enamel remineralized by the application of CPP-ACP is more resistant to alterations in pH.⁸
Combatting caries around orthodontic brackets
The efficacy of fluoride varnish containing CPP-ACP in the prevention of carious lesions around orthodontic brackets was tested using two fluoride varnishes: Duraphat and MI Varnish. Brackets were bonded to 120 bovine incisors that were then subjected to pH cycling. The pH cycling protocol required neutral saliva at 7.0 pH for two hours, followed by 4.5 pH demineralizing saliva for 22 hours. Optical coherence tomography was used to evaluate the enamel microstructure following pH cycling. The results showed that the groups treated with MI Varnish resulted in statistically shallower carious lesion depth compared to Duraphat.⁸
In another study, 33 orthodontic patients received MI Varnish on the day of bracket bonding, while 29 control group participants followed routine oral hygiene regimens. Participants were recalled at four weeks (twice) and then at three-month intervals. When patients were evaluated for the prevention of white spot formation, it was found that there was a small, but statistically significant, decrease in enamel decalcification index scores in the anterior zone of the MI Varnish group.9
Enamel demineralization during orthodontic treatment was also the subject of a double-blind study conducted by Robertson et al. in 2011, in which 60 routine orthodontic patients used either a topical tooth cream containing fluoride and CPP-ACP (MI Paste Plus, GC America) or a placebo paste in a fluoride tray for three to five minutes at night after brushing. Patients were followed at four-week recall appointments for three months. The patients using the cream with fluoride and CPP-ACP had a 53.5% reduction in enamel decalcification index scores compared to the placebo group, which had scores that increased by 91.1% over the course of the study.
The researchers concluded that the application of fluoride and CPP-ACP prevented the development of new white spot lesions in the orthodontic patients and reduced those already present on gingival and incisal surfaces.10
Enamel acid resistance
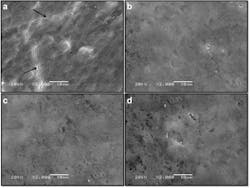
Forty primary incisors and 40 primary molars were obtained to assess the efficacy of fluoride varnish with added CPP-ACP treatments on acid resistance. The groups for this study included: control (no treatment), MI Varnish, Clinpro White Varnish, and Colgate Duraphat Varnish. After application of the fluoride varnish, the specimens were stored in a moist environment for 24 hours. The varnish was then thoroughly removed, and the specimens were immersed in a demineralizing solution with a pH of 4.4 for six hours. Next, they were rinsed, dried, and immersed in a remineralizing solution with a 7.0 pH. Lesion depth and microhardness were then analyzed by Tukey’s test and ANOVA (analysis of variance).
Conclusion
Dental caries is perhaps the most common—yet preventable—chronic disease. It can negatively impact an individual’s overall health, ability to eat, and self-esteem. It has been shown that fluoride is essential in preventing tooth decay. Fluoride-containing toothpastes, mouth rinses, and varnishes have been found to be effective adjuncts for dental caries control. Fluoride varnishes, especially those with added CPP-ACP, are particularly beneficial because of their longer contact time.
This article presented a comparison of fluoride treatments and the distinct advantages of CPP-ACP in terms of preventing demineralization, decreasing the progression of carious lesions, and potential remineralization of enamel.
Editor’s note: This article is supported by GC America. The content has been reviewed for editorial integrity per RDH guidelines. For more information on our editorial standards, visit rdhmag.com/page/ submission-guidelines.
References
- Preventing tooth decay. Centers for Disease Control and Prevention. Office of the Associate Director for Policy and Strategy. Updated May 29, 2015. Accessed September 28, 2020. https://www.cdc.gov/policy/hst/statestrategies/oralhealth/
- Shen P, Bagheri R, Walker GD, et al. Effect of calcium phosphate addition to fluoride containing dental varnishes on enamel demineralization. Aust Dent J. 2016;61(3):357-365. doi:10.1111/adj.12385
- About MI Varnish. GC America Inc. Accessed September 28, 2020. http://www.gcamerica.com/MI_Varnish/about.php
- Caperila L. ACP: Navigating our way through calcium phosphate technologies. DentistryIQ. January 19, 2011. Accessed August 31, 2020. https://www.dentistryiq.com/dental-hygiene/student-hygiene/article/16357259/acp-navigating-our-way-through-calcium-phosphate-technologies
- Tung MS. ACP technology: Amorphous calcium phosphate forming fluoride varnishes. Paffenbarger Research Center. American Dental Association Foundation. National Institute of Standards & Technology. Accessed August 31, 2020. https://www.ada.org/~/media/ADA/Education%20and%20Careers/Files/19-using_acp_to_prevent_ecc-tung_b.pdf
- MI Varnish™ with RECALDENT™ (CPP-ACP). Oral Health crc. 2014. Accessed August 31, 2020. https://oralhealthcrc.org.au/content/mi-varnish%E2%84%A2-recaldent%E2%84%A2-cpp-acp
- Panich M, Poolthong S. The effect of casein phosphopeptide–amorphous calcium phosphate and a cola soft drink on in vitro enamel hardness. J Am Dent Assoc. 2019;140(4):455-460. doi:10.14219/jada.archive.2009.0195
- Pithon MM, dos Santos MJ, Andrade CSS, et al. Effectiveness of varnish with CPP–ACP in prevention of caries lesions around orthodontic brackets: an OCT evaluation. Eur J Orthod. 2015;37(2):177-182. doi:10.1093/ejo/cju031
- Kau CH, Heiss M, Abou-kheir N, et al. Fluoride varnish with CPP-ACP reduces white-spot lesions in orthodontic treatment. IADR/PER General Session. July 26, 2018. London, England. Presentation ID 1338.
- Robertson MA, Kau CH, English JD, Lee RPm Powers J, Nguyen JT. MI Paste Plus to prevent demineralization in orthodontic patients: a prospective randomized controlled trial. Am J Orthod Dentofacial Orthop. 2011;140(5):660-668. doi:10.1016/j.ajodo.2010.10.025
- Tuloglu N, Bayrak S, Tunc ES, Ozer F. Effect of fluoride varnish with added casein phosphopeptide–amorphous calcium phosphate on the acid resistance of the primary enamel. BMC Oral Health. 2016;16(1):103. doi:10.1186/s12903-016-0299-4
About the Author

Malaina Rogers, RDH
MALAINA ROGERS, RDH, graduated magna cum laude from Briarcliffe College with an associate in applied science in dental hygiene degree in 2017. Upon completion of her hygiene degree, she continued her education, becoming certified in the use of soft-tissue diode lasers through the International Center for Laser Education program. Currently practicing minimally invasive dental hygiene in Hewlett, New York, Rogers uses her skills and relevant dental technology to improve her patients’ oral health.