Protected by a safe RDA: Setting the record straight about toothpaste abrasivity

By Pamela Maragliano-Muniz, DMD

Dental professionals hear a lot of opinions about toothpaste abrasivity. There are misunderstandings about the meaning of relative dentin abrasion (RDA) values and what they convey about the safety of a toothpaste. It can be difficult to distinguish fact from fiction. For example, a common misperception is that a toothpaste with an RDA below 100 is safer than one with an RDA of 200. This just isn't true. The fact is that a toothpaste with an RDA of 250 is just as safe as a toothpaste with an RDA of 0-249. Any toothpaste with an RDA of ≤250, the recognized threshold for safety, is safe for a lifetime of use.
The concern about toothpaste abrasivity is related to tooth wear, an important issue that has gotten quite a bit of attention lately. Tooth wear is multifactorial, and toothpaste abrasives play only a small role in the process compared to other contributing factors. The purpose of this article is to explore the role of abrasives in dentifrice, describe the test that measures toothpaste abrasivity and how these results should be interpreted, and outline implications for clinical practice.
Plaque/Stain Removal
Abrasives have been included in toothpaste formulations for generations to serve an important purpose-to remove dental plaque and surface stains during toothbrushing. As such, they're an important tool for delivering overall oral health and tooth appearance. Their major cleaning effects are due to the mechanical action of the abrasives on the surface of the teeth.1 Examples of common abrasives include hydrated silica, calcium carbonate, sodium metaphosphate, alumina and dicalcium phosphate dihydrate.
Removal of dental plaque is important to help prevent the progression of various plaque-related diseases. Dental plaque is an organized community of many different microorganisms that forms itself into an almost colorless, sticky biofilm and is found on the surface of the tongue and all hard surfaces in the oral cavity. It can vary from being comprised of totally healthy microorganisms (commensals) to being very harmful (pathogenic), predisposing the patient to dental caries, gingivitis, or periodontal diseases. If not mechanically removed on a regular basis, such as with the use of abrasive-containing toothpaste, dental plaque can calcify and form calculus deposits.
In addition to removing plaque build-up more efficiently, proper tooth brushing with an abrasive-containing toothpaste is effective at removing tooth stain related to various foods, beverages, and tobacco products. It's suggested to brush regularly, preferably on a twice-daily basis, for two minutes to minimize the build-up of stain. If not removed on a regular basis, extrinsic tooth stain can attach more firmly to the tooth surface, to the point that a prophylaxis may be required for its removal.
Measuring Abrasivity
In the early 1900s, there were no standards for the content of tooth-cleaning powders, some of which contained sand or ground cuttlefish bones as abrasives. These compounds, which would measure abrasivity in the 1,000s of RDA units by contemporary standards, were extremely damaging to tooth enamel and dentin.
In the decades that followed, methods were developed to evaluate the abrasivity of toothpaste formulations in the laboratory. A landmark study in 1948 assessed the abrasivity of toothpaste formulations relative to cleaning performance.2,3 Kitchin & Robinson4 found that over 90% of stain removal could be achieved with toothpaste abrasivity that produced less than 1 mm of dentin wear per 100,000 brush strokes, as assessed using an automated simulation of brushing. The use of dentin as the test substrate was also established during this era. Dentin is much softer than enamel, which makes it considerably easier to use for testing the relative abrasivity of different toothpaste formulations.
Figure 1: Cleaning efficacy as a function of RDA.
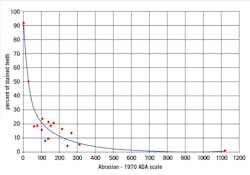
Figure 2: Non-carious cervical lesion commonly associated with abrasion, excessive occlusal forces, and a low pH.

In 1976, the American Dental Association published the RDA method, which became the standard for laboratory measurement of toothpaste abrasiveness that is still used today.5 RDA values are obtained in the laboratory by comparing the amount of dentin tooth structure worn away by a standardized tooth brushing protocol using any given toothpaste compared to a standard reference abrasive assigned an RDA value of 100. By 1995, the International Standards Organization (ISO) had adopted this method as an international standard for measuring toothpaste abrasivity. The standard brushing protocol prescribes factors such as pressure, time, temperature, and humidity. The ISO specification states that a toothpaste should not exceed an RDA of 250, which is considered the safe limit for hard tissues, and that toothpaste with an RDA value below 250 is safe for daily use. This upper limit of "250" is 2.5 times the abrasiveness of the reference standard. Since the ISO and ADA standards were established, the industry has largely self-regulated and toothpastes with an RDA value over 250 have been removed from the market. The ISO standards ensure that all products for sale meet the standards for safety.
What do RDA values mean?
Stain removal-There is typically a much lower stain removal benefit for toothpastes with RDA values less than 100 compared to those with values greater than 100. Once you exceed an RDA value of 250, there is little incremental stain removal benefit (see Figure 1).
Dentin wear-A prevailing belief is that a lower RDA value is safer and there have been claims that an RDA value over 150 is considered unsafe. There is no clinical basis for this assertion and this "information," most commonly accessible on the internet, is incorrect and misleading. Clinical studies looking at the difference in dentin wear between toothpastes with various RDA levels below 250 have not shown a significant difference in wear.6,7 Toothpastes should be considered as either "less than" or "more than" the RDA upper limit of 250-like a "pass/fail" test. There are no degrees of safety below 250.
Abrasive potential under extreme laboratory conditions-It's important to note the RDA method was not originally developed to compare toothpastes, but rather to compare products to a reference standard of 100.8 The test is an indication of the abrasive potential of a toothpaste as tested under laboratory conditions, which are much more extreme than typical everyday brushing.
For example, the RDA test does not include pellicle, which plays a major role in protecting the teeth from wear processes in real life. Furthermore, the RDA method generally includes 1,500 continuous, horizontal manual toothbrush strokes, which is equivalent to approximately two months of brushing all at once. Most patients only spend about 5 seconds brushing each tooth surface and under these conditions the protective pellicle is not removed.
Factors Behind Tooth Wear
Tooth wear is a process resulting from three primary factors-abrasion (from the interaction of teeth with other materials); attrition (from tooth-to-tooth contact); and erosion (wear after teeth come into contact with environmental or dietary acids) (see Figures 2-5). In addition, numerous behaviors and health factors contribute to the process of tooth wear, including, but not limited to: a diet high in acidic beverages and foods, bruxism, aggressive or improper tooth brushing, low pH of the oral cavity (acid reflux, GI disorders, bulimia nervosa) and oral hygiene habits.
Relative to these factors, tooth brushing with abrasive-containing toothpaste by itself causes minimal wear.
In one published survey of 100 consecutive cases of problematic tooth wear referrals, detailed histories were taken of each case to determine the etiology of tooth wear. Fifty-eight percent of cases were attributed to erosion alone or erosion combined with another etiology.
No cases could be attributed to abrasion alone.9
In a recent paper that discussed clinical and experimental findings regarding the interactions between attrition, abrasion and erosion in tooth wear, the authors stated, "It has been concluded that normal toothbrushing habits with toothpastes that conform with the ISO standard will, in a lifetime's use, cause virtually no wear of enamel and clinically insignificant abrasion of dentine."10
Figure 3: Attrition indicative of bruxism.

Figure 4: Erosion suggestive of untreated acid reflux or bulimia.

Implications for Patients
So what's the bottom line for patient care? Toothpastes with an RDA of 250 or less are safe for a lifetime of use, and virtually all modern toothpastes meet this standard. Patients can mitigate their risk for tooth wear with proper oral hygiene and technique. Power toothbrushes, particularly those with a pressure sensor, can reduce aggressive brushing, and the use of Bluetooth technology in combination with certain power brushes has given patients even more tools for monitoring and getting feedback on their brushing techniques.
Another important step to help patients reduce tooth wear is evaluating dietary habits, overall health, and lifestyle behaviors. Factors that increase the risk of tooth wear include a diet rich in acidic foods and beverages (citrus fruits and red wine, for example), gastroesophageal reflux disorder, and/or bruxism. Toothpaste containing stabilized stannous fluoride (Crest Pro-Health, for example) has been shown to be significantly more protective than other types of fluoride dentifrices against dental erosion, a factor in tooth wear.11,12
Figure 5: Erosion pattern suggests lemon sucking.

Current ADA Stance
A recent statement was released by the American Dental Association on the issue of abrasivity:13
"Although tooth enamel is the hardest substance in the body, the dentin that lies beneath it can become exposed-through, for example, wear of the enamel or gingival recession. Because of concern about abrasion of these tissues, scientists have spent decades researching and monitoring the effect of dentifrice abrasives on these tooth structures.
"To help quantify the abrasivity of dentifrices, the ADA along with various academic, industry and government agencies established a standardized scale called Relative Dentin Abrasivity (RDA). This scale assigns dentifrices a value from 0 to 250, relative to a standard reference abrasive that is arbitrarily given an RDA value of 100. All dentifrices at or below 250 RDA are considered safe and effective. In fact, clinical evidence supports that lifetime use of proper brushing technique with a toothbrush and toothpaste at an RDA of 250 or less produces limited wear to dentin and virtually no wear to enamel.
"Relative dentin abrasivity can be used by industry, researchers, or standards organizations to develop new products or to conduct quality control. It should not be used to rank the safety of dentifrices with RDA values below 250. These values do not respond to potential clinical effects, like abrasion.
"The RDA testing method and the upper limit of 250 has been adopted by the International Standards Organization (ISO) and is included in the manufacturing standards, ISO Toothpaste Specification 11609. All dentifrices with the ADA Seal of Acceptance have an RDA of 250 or less."
Pamela Maragliano-Muniz, DMD, is an editorial director for Pearls for Your Practice: The Product Navigator, an e-newsletter from DentistryIQ and Dental Economics. She was a dental hygienist before earning her DMD from Tufts University School of Dental Medicine and her certificate in advanced prosthodontics from the UCLA School of Dentistry. She teaches, and she maintains a private practice in Salem, Mass. In 2010, her practice was named the Adult Preventive Care Practice of the Year by the American Dental Association.
Here are the three key takeaways about toothpaste abrasivity:
- Abrasive compounds are important to remove stain and to efficiently remove plaque during toothbrushing.
- The RDA test is an indication of the abrasive potential of a dentifrice as tested under laboratory conditions, which are more extreme than typical everyday brushing. A toothpaste with an RDA equal to or under 250 is safe for a lifetime of use.
- It's important to assess patients for all tooth wear risk factors; relative to erosion and attrition, toothpaste abrasivity plays a small role in tooth wear.
References
- Dörfer CE. (2010) Abrasivity of dentifrices from a clinical perspective. J Clin Dent. 21 (Suppl): S4.
- St. John S, White DJ. (2015) History of the development of abrasivity limits for dentifrices. J Clin Dent. 26 (2): 50-54.
- Hefferren J. (2010). Critical points in the evolution of laboratory methods to measure the functionality of toothpastes. J Clin Dent. 21 (Suppl): S6-S10.
- Hitchin PC, Robinson HBG. (1948) How abrasive need a dentifrice be? J Dent Res. 27;501-506.Hefferren JJ. (1976) A laboratory method for assessment of dentifrice abrasivity. J Dent Res. 55 (4): 563-73.
- Saxton CA, Cowell CR. (1981) Clinical investigation of the effects of dentifrices on dentin wear at the cementoenamel junction. J Am Dent Assoc.102 (1):38-43.
- Volpe AR, Mooney R, Zumbrunnen C, Stahl D, Goldman HM. (1975) A long term clinical study evaluating the effect of two dentifrices on oral tissues. J Periodontol. 46 (2):113-8.
- González-Cabezas C. (2010) Determination of the abrasivity of dentifrices on human dentin using the radioactive (also known as relative) dentin abrasion (RDA) method. J Clin Dent. 21 (Suppl): S9.
- Smith BG, Knight JK. A comparison of patterns of tooth wear with aetiological factors. Br Dent J. 1984 Jul 7;157(1):16-9.
- Shellis RP, Addy M. (2014) The interactions between attrition, abrasion and erosion in tooth wear. In: Lussi A, Ganss E (eds): Erosive Tooth Wear. Monogr Oral Sci. Basel, Karger 25:32-45.
- Hancocks SJ. (2014) Stabilised stannous fluoride and dental erosion. Int Dent J. 64:1-50.
- Carvalho TS, Colon P, Ganss C, et al. (2015) Consensus report of the European Federation of Conservative Dentistry: erosive tooth wear-diagnosis and management Clin Oral Inv. 19, (7): 1557-1561.
- http://www.ada.org/en/member-center/oral-health-topics/toothpastes