Nitrous oxide and oxygen analgesia: A strong safety record supports option in pain control

By Laura Webb, RDH, MS, CDA
Nitrous oxide-oxygen (N2O-O2) has been safely used for sedation in dentistry for decades. Its primary use today is for anxiety management, since fear and anxiety are associated with lowered pain threshold and increased patient discomfort. As early as 1971, (Washington State) dental hygienists have been able to provide N2O-O2 analgesia. It is interesting that only 32 states currently allow hygienists to administer it, even though it is incredibly safe and easy to use. Dental hygienists are usually certified to provide “conscious sedation” analgesia, requiring that throughout procedures the patient should remain conscious, breathe normally, be responsive to verbal communication, and their cough and gag reflexes functioning normally.
Patients often avoid dental treatment because of their fear of pain and/or receiving local anesthesia (“the needle”). Since N2O-O2 has the ability to raise the patient’s pain threshold and reduce anxiety, N2O-O2 analgesia has great value during the provision of local anesthesia for definitive debridement procedures.

I find that once the local anesthetic has been provided, the percentage of N2O often can be reduced. Although N2O-O2 does not replace the need for local anesthesia, the analgesic properties of it can help patients to become calm and relaxed to the extent that simple procedures, such as probing or periodontal maintenance procedures, performed in the presence of inflammation, may be more comfortable and may not, therefore, require the use of local anesthesia.
Some patients also fear or are annoyed by power scaling procedures and the use of N2O-O2 can help alleviate their discomfort as well as their gag reflex. In addition, patients often report not remembering any discomfort or the duration of procedures - time seems to pass more quickly.
Strong safety record
N2O-O2 has an impressive 150-year safety record, which is related to the properties of the gases, administration technique (titration), and equipment fail-safe devices. The literature reports that there has never been a death attributed to it when used properly as the sole sedative.1-3 With adequate training and proper technique, complications are very rare. No allergies have been reported; there are few side effects; and there are virtually no adverse effects on liver, kidneys, brain, cardiovascular system, or respiratory system (see COPD exception below).1-5
Recall that patients who are medically compromised require excellent pain control to avoid exacerbation of their conditions as a result of stress from pain or anxiety. N2O-O2 reduces anxiety for these patients which facilitates safe provision of local anesthesia. Patients with cardiovascular disease benefit from stress reduction protocols and may also require a reduced dose of epinephrine.6 The use of N2O-O2 can be particularly advantageous for these patients because not only does it reduce anxiety and raise the pain threshold (facilitating safety during local anesthesia), but it increases the diameter of blood vessels, improving the cardiac blood flow.1-6 N2O-O2 does not irritate respiratory mucosa and so it is considered safe for patients with asthma (except during an attack), and may actually lower the risk of an asthma attack because it reduces the stress associated with provoking an attack.1-5
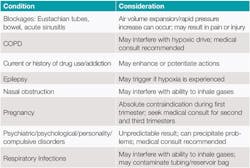
There are few contraindications to N2O-O2 analgesia for patients who would normally qualify for elective procedures such as nonsurgical periodontal therapy. The opinions of experts regarding identifying and classifying contraindications to N2O-O2 as absolute versus relative varies a bit. Some authors state there are no absolute medical contraindications; others feel there are a few, while still others feel that there are several absolute contraindications. A medical consult is advised for patients with complex medical conditions or recent eye surgeries. Table 1 briefly identifies several commonly listed contraindications found in the literature.
We often provide treatment for patients with a chronic obstructive pulmonary disease (COPD), which represents a relative contraindication to the provision of N2O-O2 analgesia. Simply stated, this is because these patients can present with chronically elevated CO2 levels in their blood and are stimulated to breathe by lowering O2 levels, as opposed to elevated CO2 levels. These patients’ stimulus to breathe may be negatively impacted due to the increase of O2 levels provided during N2O-O2 analgesia. A medical consultation is recommended prior to administration.1-5
Standard of care
The fact that the depth and duration of sedation is easily controlled by the clinician is an important safety feature. The standard of care requires utilization of the titration technique that contributes to avoiding over-sedation. This technique, which begins with 100% O2, is the provision of small, incremental doses (adding N2O and subtracting O2) slowly until the baseline for the patient is reached.
If the patient feels that he or she is receiving too much nitrous, the gases can be quickly adjusted and the patient will feel relief almost immediately. Large fluctuations, up and down, of N2O may result in patient discomfort, including nausea, and should be avoided. The patient should receive 100% O2 after the termination of N2O for a minimum of five minutes.1 Since N2O is not metabolized in the body and 99.9% is eliminated unchanged via exhalation, it is rapidly eliminated after administration, within three to five minutes.2,3

Figure 1: Porter Double mask
Image courtesy of Porter Instrument, Parker Hannifin Corporation, Hatfield, PA.
However, the recovery time for patients varies, and there are differing opinions in the literature regarding the amount of time and evaluations required for recovery. It becomes the clinician’s responsibility to ascertain recovery time for each patient.1
There are several equipment safety devices, including color-coded tanks, tubing, outlets, flowmeters and pressure gauges, a pin indexing system, a diameter indexing system, oxygen depletion indicators, alarms, locks, automatic minimal oxygen levels, and fail-safe devices such as automatic N2O shut-off if O2 flow is interrupted.

Figure 2: Porter Silhouette mask
Image courtesy of Porter Instrument, Parker Hannifin Corporation, Hatfield, PA.
The standard of care also requires utilization of a properly operating scavenging system to lower the risk of exposure of trace N2O to office personnel. Scavenging nasal hoods come in a variety of designs (see Figures 1-3). To protect against cross-contamination, nasal masks should be sterilizable or disposable. The N2O-O2 equipment should also be leak-tested regularly and monitoring devices are available to detect operator and staff exposure to waste gas.
N2O-O2 analgesia has become very popular for anxiety reduction. Although it is not indicated for all patients, it may be especially appropriate for dental hygiene patients who present with mild to moderate anxiety, mild inflammation, intolerance for long appointments, cardiovascular conditions, or asthma.

Figure 3: Safe Sedate mask system
Image courtesy of Safe Sedate
Licensed to provide both local anesthesia and N2O-O2 analgesia since 1980, I have had the good fortune of working with several periodontists and general dentists who had it available in every operatory via a central gas supply system which made it very convenient for me to use, as needed. I have found N2O-O2 analgesia to be very safe and effective, particularly during provision of local anesthesia and nonsurgical periodontal therapy (NSPT).
Through teaching and working in private practice settings, I have learned that even the most experienced clinicians should take time to frequently reassess their skills and stay current with the standard of care, equipment, and techniques. The Clark & Brunick text listed among the references below, provides particularly useful, detailed content as it is dedicated to the topic of N2O-O2 sedation. The provision of N2O-O2 analgesia for patients is not difficult, but it does require maintenance of skill, attention to safety issues, and evidence-based practice. RDH
References
1. Clark MS, Brunick, AL. (2015) Handbook of Nitrous Oxide and Oxygen Sedation 4th ed. Elsevier.
2. Malamed SF. (2009) Sedation: A Guide To Patient Management, 5th ed. Chapter 12. Elsevier.
3. Donaldson M. (2016) Nitrous Oxide-Oxygen Inhalational Sedation: Managing Pain & Anxiety. SC Publishing; www.westernschools.com.
4. Shuman I. Nitrous oxide: use and safety. www.dentaleconomics.com, May 2016.
5. Darby M, Walsh M. (2015) Dental Hygiene Theory and Practice 4th ed. Chapter 41. Elsevier.
6. Toile SL, Walters AN. Dental care for patients with heart disease. Dimensions of Dental Hygiene. April 2015;13(4):65-68.
LAURA J. WEBB, RDH, MS, CDA, is an experienced clinician, educator, and speaker who founded LJW Education Services (ljweduserv.com). She provides educational methodology courses and accreditation consulting services for allied dental education programs and CE courses for clinicians. Laura frequently speaks on the topics of local anesthesia and nonsurgical periodontal instrumentation. She was the recipient of the 2012 ADHA Alfred C. Fones Award. Laura can be contacted at [email protected]