Ecological drivers of oral dysbiosis and disengagement in adolescents

Adolescent patients commonly present with persistent plaque biofilm, recurrent dental caries, and reduced engagement with oral hygiene recommendations. These patterns are frequently attributed to inadequate motivation; however, increasing evidence supports an ecological model of oral disease in which microbial behavior is influenced by dietary, hormonal, and airway-related factors.
This article describes a representative adolescent clinical presentation in which phase-contrast microscopy was used as an ecological assessment tool, revealing a dense, Candida-favoring oral biofilm despite average reported hygiene practices. The findings are discussed in the context of three interacting contributors frequently observed during adolescence: frequent exposure to fermentable carbohydrates, pubertal hormonal changes, and mouth breathing–associated alterations in salivary function. These converging factors promote biofilm persistence and resistance to mechanical disruption, potentially contributing to patient frustration and disengagement.
By reframing adolescent oral disease through a biologically informed, ecological lens, clinicians may better identify underlying contributors, guide targeted preventive strategies, and improve long-term patient engagement in oral health care.
Introduction
Most dental professionals have encountered adolescent patients with visibly heavy biofilm, inconsistent oral hygiene, and recurrent caries despite repeated instruction. Clinical encounters often follow a predictable pattern: another cavity, another reminder to brush and floss more effectively, and increasing frustration on both sides of the chair. Over time, many adolescents exhibit disengagement that may be misinterpreted as apathy or noncompliance.
Closer evaluation through a biological and ecological lens often reveals a more complex explanation. The mouth, particularly during adolescence, may reflect systemic, hormonal, and airway-related influences that render conventional hygiene strategies insufficient. Contemporary oral biology increasingly supports an ecological understanding of dental disease, in which microbial behavior is shaped by environmental conditions rather than motivation alone.1
Ecological findings under phase-contrast microscopy
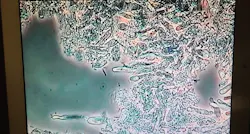
This perspective is informed by repeated clinical observations of adolescent patients whose plaque biofilm was evaluated using phase-contrast microscopy as an ecological assessment tool. In a case involving a 15-year-old female presenting with average adolescent oral hygiene (no extreme behaviors or overt pathology were initially apparent), microscopic evaluation revealed numerous oval and elongated structures consistent with yeast morphology, along with forms suggestive of budding and early pseudohyphae behavior. The biofilm appeared dense, matted, and poorly mobile, with areas of stagnation indicative of reduced oxygen tension and acidic conditions.
Phase-contrast microscopy does not diagnose specific microbial species; however, it is well suited for identifying ecological patterns within plaque biofilm. From an oral microbiology standpoint, this constellation of findings is consistent with a Candida-favoring oral environment, a phenomenon increasingly recognized as part of the normal oral mycobiome when ecological conditions permit fungal dominance.2,3
The Candida triangle in adolescents
In adolescent patients, Candida-dominant biofilm patterns are rarely attributable to hygiene practices alone. Instead, they typically arise from the interaction of dietary substrate exposure, pubertal hormonal changes, and airway-related salivary dysfunction.
Dietary substrate exposure
Teen diets often involve frequent exposure to refined carbohydrates, even in the absence of overt sugar consumption. Crackers, chips, granola bars, sports snacks, and flavored beverages all contribute fermentable substrates to the oral cavity. Salivary amylase rapidly converts starches into sugars directly at the tooth surface, increasing biofilm adhesion and metabolic activity. Under these conditions, Candida exhibits enhanced adhesion and persistence, while acidogenic bacteria contribute to stabilization of thick, tenacious plaque.1,4
Pubertal hormonal influences
Puberty represents a period of significant hormonal fluctuation that directly impacts oral tissues and microbial behavior. Estrogen has been shown to enhance Candida adhesion to mucosal surfaces, while epithelial permeability and immune signaling remain in developmental flux. Similar biologic vulnerability is observed during pregnancy and later during perimenopause, suggesting a shared hormone–microbe interaction across life stages.2,3
Mouth breathing and salivary dysfunction
Mouth breathing, particularly during sleep, further accelerates ecological imbalance. Evaporation of saliva reduces buffering capacity, lowers oral pH, and promotes formation of thick, adherent biofilm.
Saliva plays a critical protective role in maintaining oral tissue health and microbial balance, and reduced salivary flow or altered composition significantly increases disease susceptibility.5 Candida thrives in acidic, low-oxygen environments, making mouth breathing a powerful yet often overlooked contributor to adolescent oral dysbiosis. Airway-related factors, including sleep-disordered breathing, have been shown to alter oral and craniofacial physiology in pediatric populations.6
Editor's note: This article appeared in the June 2026 print edition of RDH magazine. Dental hygienists in North America are eligible for a compiimentary print subscription. Sign up here.
Reframing “poor oral hygiene” in adolescents
Within this biological context, behaviors often labeled as poor oral hygiene are more accurately understood as downstream effects rather than primary causes. When the oral terrain favors Candida dominance, plaque forms rapidly, adheres aggressively, and resists mechanical disruption. Recolonization occurs quickly, limiting the effectiveness of manual brushing alone.
In tweens and teens, the dexterity, consistency, and attention to detail required for complete plaque removal are still developing. When repeated effort fails to produce visible improvement, frustration at never performing oral care “correctly” may settle in. Over time, many adolescents disengage—not because they lack concern, but because the biological challenge exceeds their current capacity to manage it.
Psychological disengagement and clinical consequences
Adolescent resignation represents a critical yet underrecognized factor in disease progression. When effort does not translate into improvement, disengagement becomes a rational response rather than a behavioral flaw. This withdrawal is frequently misinterpreted as noncompliance, leading to further erosion of trust and motivation.
The emotional consequences of this dynamic are clinically significant. Adolescents who disengage from preventive care are at increased risk for accelerated caries development, persistent gingival inflammation, orthodontic complications, and long-term oral health challenges.4,7
Healing the mouth by supporting the body
Sustainable improvement in adolescent oral health requires addressing the systemic factors that shape oral ecology. Healing begins with adequate nutrition, including sufficient protein intake to support tissue repair and immune signaling, along with reduction of refined starch exposure and constant sipping of sweetened beverages that perpetuate oral sugar availability.
Restorative sleep supports immune regulation, hormonal balance, and salivary flow, while airway optimization through nasal breathing helps preserve saliva’s protective functions.5,6 Body chemistry also plays a critical role. Vitamin D status, mineral balance, hydration, and metabolic regulation influence saliva quality, tissue resilience, and enamel integrity.8
Clinical implications and a new conversation
This ecological perspective challenges the assumption that adolescent oral disease reflects indifference or poor motivation. Instead, it highlights a hormonally primed, carbohydrate-fed, mouth-breathing oral ecosystem that favors fungal persistence and biofilm stability.
Shifting the clinical conversation from “brush better” to “let’s change the environment” restores agency, dignity, and engagement. Recognizing oral disease as biologic communication rather than behavioral failure allows clinicians to intervene earlier and more effectively.
Conclusion
In pediatric and adolescent dentistry, the mouth often communicates systemic imbalance long before overt disease becomes entrenched. By listening early and addressing the biological drivers of dysbiosis, clinicians may prevent disease progression and preserve adolescents’ long-term relationship with oral health.
AI assistance disclosure: AI-assisted tools were used for language refinement and editorial support. All clinical observations, interpretations, and conclusions are those of the author, who retains full responsibility for the content.
Conflict of interest statement:The author declares no conflicts of interest relevant to this article.
References
-
Kleinberg I. A mixed-bacteria ecological approach to understanding the role of the oral bacteria in dental caries causation: an alternative to Streptococcus mutans and the specific-plaque hypothesis. Crit Rev Oral Biol Med. 2002;13(2):108-25. doi:10.1177/154411130201300202
-
Krom BP, Kidwai S, Ten Cate JM. Candida and other fungal species: forgotten players of healthy oral microbiota. J Dent Res. 2014;93(5):445-51. doi:10.1177/0022034514521814
-
Samaranayake L, Matsubara VH. Normal oral flora and the oral ecosystem. Dent Clin North Am. 2017;61(2):199-215. doi:10.1016/j.cden.2016.11.002
-
Gussy MG, Waters EG, Walsh O, et al. Early childhood caries: current evidence for aetiology and prevention. J Paediatr Child Health. 2006;42(1-2):37-43. doi:10.1111/j.1440-1754.2006.00777
-
Dawes C. Salivary flow patterns and the health of hard and soft oral tissues. J Am Dent Assoc. 2008 May;139 Suppl:18S-24S. doi:10.14219/jada.archive.2008.0351
-
Villa MP, Rizzoli A, Miano S, et al. Efficacy of rapid maxillary expansion in children with obstructive sleep apnea syndrome: 36 months of follow-up. Sleep Breath. 2011;15(2):179-84. doi:10.1007/s11325-011-0505-1
-
Petersen PE. The World Oral Health Report 2003: continuous improvement of oral health in the 21st century—the approach of the WHO Global Oral Health Programme. Community Dent Oral Epidemiol. 2003;31 Suppl 1:3-23. doi:10.1046/j..2003.com122
-
Schroth RJ, Lavelle C, Tate R, et al. Prenatal vitamin D and dental caries in infants. Pediatrics. 2014;133(5):e1277-84. doi:10.1542/peds.2013-2215
About the Author

Barbara Tritz, MSB, BSDATE, BRDH
Barbara is a practicing biological dental hygienist at Green City Dental in Edmonds, Washington. She is the owner of Washington Oral Wellness in Kirkland, Washington, where she practices orofacial myofunctional therapy. She completed her accreditation in biological dental hygiene through the International Academy of Oral Medicine and Toxicology, and is laser certified through the Academy of Laser Dentistry. In 2019 Barbara received the HuFriedy-American Dental Hygienist Association Master Clinician Award. Barbara can be contacted at [email protected].