Tongue tie as a missing link to caries management

It is not widely known that arch expansion in the adult mouth is possible. Many dentists and orthodontists do it every day. As illustrated in Figure 1 (above), Dr. Mike Mulligan, past president of the American Academy for Oral Systemic Health, had his arch expanded by approximately 8 mm and 3 mm anterior/posterior at the age of 62. When did this arch discrepancy first appear? What could dentistry have done proactively?
Embryologic oral development notwithstanding, there are many things that dental hygienists can do to encourage oral development to reach a genetic potential, and to remove epigenetic tags that interfere with optimum growth. The findings of Dr. Weston A. Price and others showed us that the diet, not just the sugar content of the diet, can interfere with good oral development.1 Dr. Price found that the introduction of the westernized diet of processed foods and seed oils led to the first generation born into this diet developing small arches that could not maintain proper dental alignment.
What the research reveals
Dr. Marianna Evans, a double board-certified periodontist and orthodontist, and Dr. Kevin Boyd, a pediatric dentist in Chicago with a master’s degree in human nutrition, have been on an archaeological odyssey to find out when the human arch stopped accommodating a full complement of adult teeth. Different findings indicate that preindustrial skulls of infants were shaped quite differently than what appeared during the Industrial Revolution. They point out that the mandible was never in a retrusive position until industrial times.2
Dr. Christian Guilleminault, the physician who coined the term apnea hypopnea index (AHI), found in his studies that a defect in the strength of the suction during fetal life affected mandibular development and that the absence of normal suction is associated with a gutter palate. The gutter palate is a high narrow arch or a vaulted arch. We have known about the dysmorphia of the oral cavity with improper tongue placement and oral breathing for quite some time.3,4,5

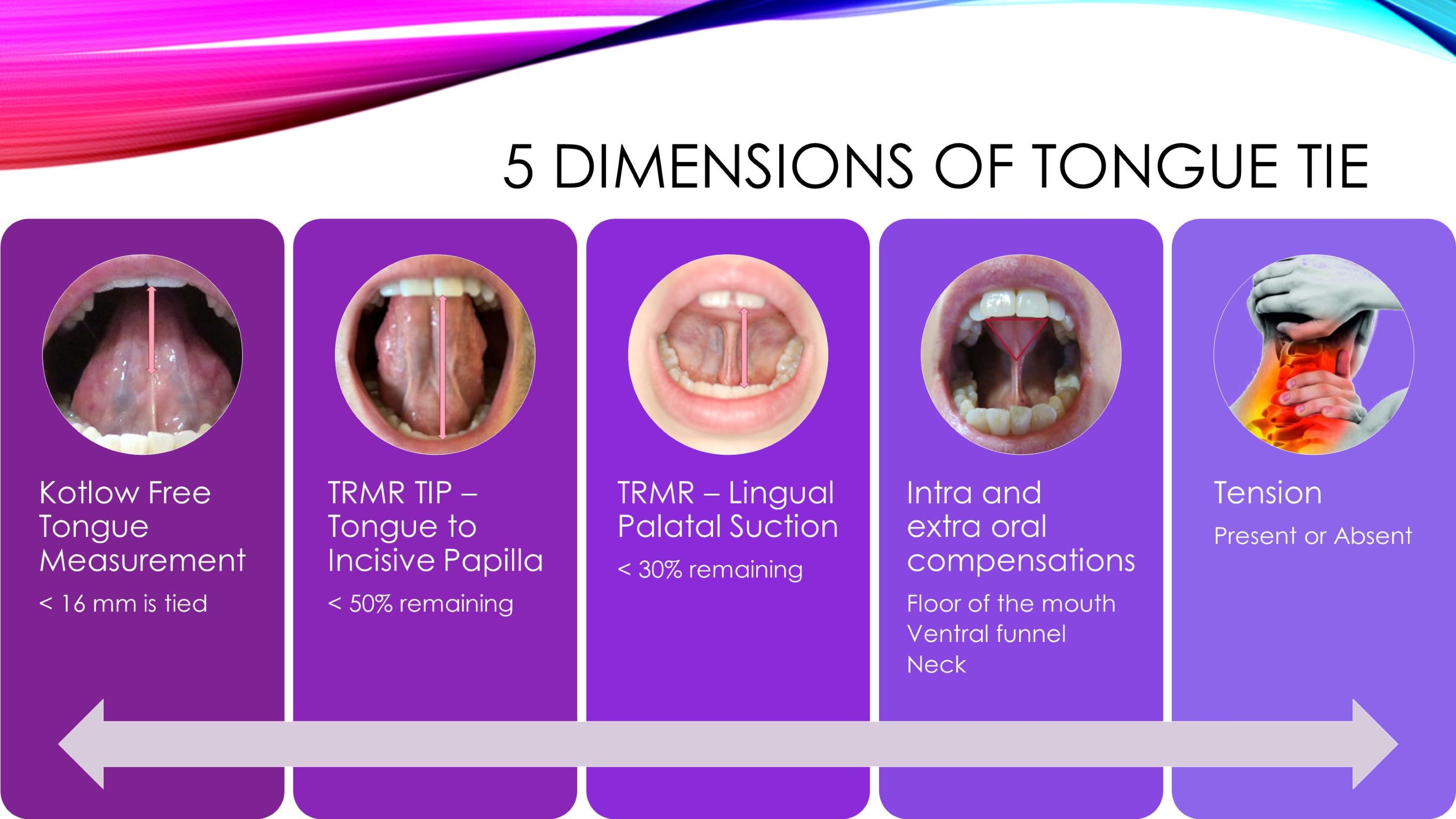
Dr. Guilleminault and others have been focusing on the mobility of the tongue as a reason for improper growth and development. Dr. Soroush Zaghi has been studying tongue mobility and has provided a framework to determine whether a tongue is tied or not. Until his current research starting in 2018, one could argue that a tongue tie was one where the tongue could not protrude past the mandibular teeth. Today we know there are five dimensions of a tongue tie, and it is worthwhile to address the tongue tie at any stage as soon as it’s noticed (figure 2).6.7
More by Shirley Gutkowski
The airways in our pediatric patients
Snoring: Challenges and solutions
How mouth taping can be key to achieving healthy nasal breathing
The importance of being proactive
We can no longer simply say, “Oh, you can talk, and you can eat, so we'll just leave it.” A restricted tongue can lead to snoring and other breathing problems. So, it's important to address it as soon as it's recognized. The malocclusion effects of a tongue tie are easily repaired by orthodontics, but why wait until malocclusion is present? In adults with poor occlusion, it may seem like it’s too late to do anything to the soft tissue. An adult with a tongue tie release has a far better quality of life due to the reduction in headache pain, migraine pain, jaw joint pain, swallowing, and a variety of other effects.8
You may be surprised to learn that a tongue restricted in the middle third, where the frenum may be short and doesn’t allow the posterior part of the tongue to lift, interferes with the dimensions of the pharyngeal and laryngeal airway. A tongue that is tied can slump into the airway, contributing to a very narrow airway that collapses easily during the paralytic sleep cycle. Substantial relief may be in the form of a mandibular advancement device.
Restricted tethered oral tissues of the tongue can contribute to dental decay. The restricted tongue that interferes with the space of the oropharynx forces open-mouth breathing. Not only does open-mouth breathing dry out the mouth during sleep, it also lowers the pH of the oral environment, which contributes to a proliferation of cariogenic bacteria.9 Saliva is a vital fluid that contributes nutrients to the teeth to maintain healthy and sound enamel.
Learning that your patient may be suffering from dental decay due to snoring may be an important key to successful caries management. An oral device to limit snoring is incredibly beneficial. However, rebuilding the enamel may need an extra kick. A referral to an orofacial myofunctional therapist can be helpful,8 to establish nasal breathing as can application of a remineralization cream before placing the appliance at night.
An orofacial myofunctional therapist will look at the function of the tongue and determine whether the tongue is truly restricted. This may be the root cause to dental decay. The mandibular advancement device may be the solution to snoring if the patient is comfortable wearing one. A remineralization cream like Remin Pro (Voco) can provide care to the enamel and keep it from further breakdown, as well as provide the enamel with needed minerals for self-repair.
A remineralization cream as a salve on the teeth before seating the snoring device bathes the teeth in appropriate minerals. The nano-hydroxyapatite (calcium and phosphate) molecules in the Remin Pro fit into the missing parts of the enamel. There is no need for the molecules to reassemble before repairing the microscopic breakdown of the enamel.
Dental professionals have an obligation to help patients retain their teeth for a lifetime. Asking patients to take full responsibility for their own disease is not practical or fair. They don't know what they don't know; we’re obligated to provide them with the products and information they need to make appropriate decisions. Children who present with restricted tongues and who have been in speech therapy for years with no progress likely have a tongue tie. This can impede swallowing and breathing and contribute to sleep disordered breathing throughout life.
Addressing problems in children is preferable. Adult arch expansion is possible for the right case presentation. But it is expensive and not for everyone. An adult mandibular advancement device coupled with Remin Pro can improve dental outcomes as well as reduce snoring.
Voco is a financial supporter.
Editor's note: This article appeared in the September 2022 print edition of RDH magazine. Dental hygienists in North America are eligible for a complimentary print subscription. Sign up here.
References
- Diet in relation to dental caries. Weston Price. February 16, 2016. https://www.westonaprice.org/health-topics/dentistry/diet-in-relation-to-dental-caries/#gsc.tab=0
- Boyd KL. Darwinian Dentistry part 1. An evolutionary perspective on the etiology of malocclusion. Dentistry for Children. http://www.dentistry4children.net/assets/site/files/JAOSn-d11_Boyd_finalREV%5B1%5D.pdf
- Löfstrand-Tideström B, Hultcrantz E. The development of snoring and sleep related breathing distress from 4 to 6 years in a cohort of Swedish children. Int J Pediatric Otorhinolaryngology, 2007;71(7):1025–1033. https://doi.org/10.1016/j.ijporl.2007.03.005
- Srinivasan B, Chitharanjan AB. (2013). Skeletal and dental characteristics in subjects with ankyloglossia. Prog Ortho. 2013;14(11):44. doi:10.1186/2196-1042-14-44
- Yoon AJ, Zaghi S, Ha S, Law CS, Guilleminault C, Liu, SY. Ankyloglossia as a risk factor for maxillary hypoplasia and soft palate elongation: A functional - morphological study. Ortho Craniofacial Res. 2017;20(4):237–244. https://doi.org/10.1111/ocr.12206
- Zaghi S, Shamtoob S, Peterson C. Assessment of posterior tongue mobility using lingual-palatal suction: progress toward a functional definition of ankyloglossia. J Oral Rehab.2021;48(6):692–700. https://doi.org/10.1111/joor.13144
Zaghi S, Valcu-Pinkerton S, Jabara M, et al. Lingual frenuloplasty with myofunctional therapy: Exploring safety and efficacy in 348 cases. Laryngoscope Investig Otolaryngol. 2019;4(5):489-496. Published 2019 Aug 26. doi:10.1002/lio2.297
- Govardhan C, Murdock J, Norouz-Knutsen L. Lingual and maxillary labial frenuloplasty with myofunctional therapy as a treatment for mouth breathing and snoring. Case reports in otolaryngology. 2019;10. https://doi.org/10.1155/2019/3408053
- Davidovich E, Hevroni A, Gadassi LT. (2022). Dental, oral pH, orthodontic and salivary values in children with obstructive sleep apnea. Clin Oral Investig. 2022;26(3):2503–2511. https://doi.org/10.1007/s00784-021-04218-7
About the Author

{kind=link}
{kind=link}
Shirley Gutkowski, BSDH, RDH
Shirley Gutkowski, BSDH, RDH, is the owner and primary practitioner at Primal Air LLC, located in Sun Prairie, Wisconsin. She and her team of RDH OMTs see most of their patients online. Primal Air is a three-part practice that not only serves the needs of patients but also gives OMT-trained RDHs a place to learn and practice the science of OMT. Gutkowski can be reached at [email protected].
Updated February 3, 2022