Watch it do what?
by Charles D. Samaras, DMD
Radiographs and explorers are inaccurate in detecting early decay, and dental professionals simply guess at the outcome. Innovative technology eliminates the 'watching' and the 'guessing.'
One difficult and sometimes frustrating aspect of dentistry is the detection of initial caries in unrestored teeth. Over the years, doctors and hygienists have been limited to conventional methods of caries detection, such as radiographs and explorers, to determine if frank decay is present and a restoration is required.
As we all know, a radiograph is only an aid to diagnosis - demonstrated by the fact that decay usually has progressed further than a radiograph may indicate. Additionally, explorers range from extremely sharp to very dull. Even with sharp explorers, we are constantly asking ourselves, " Is it a stick, or not?"
What does a stick mean? Is it sound tooth structure, a deep groove, an incipient lesion, or frank decay? What do we do? Do we restore? Our sharp explorer just got a stick. If it is an incipient lesion, there is a consensus in dental circles that a sharp explorer may actually initiate cavitation of that lesion. Therefore, if we are conservative, we don't treat any small lesions. If we are aggressive, we restore all small lesions. More often than not, we are just not sure, so we say, "Watch!"
Watch it do what? Will it ever get better if we are not sure what it is or if treatment is required? I am sure there are plenty of hygienists and doctors who have placed watches on a lesion only to see full-blown decay six months later. Conversely, there have been instances where I have restored a stick only to realize that it would have been best to treat the incipient lesion with a sealant to abort the decay process.
The bottom line on initial lesions is this. Radiographs and explorers are inaccurate in detecting early decay. Many times, we are simply guessing at the outcome. When it comes to patient care, there is only one thing worse than guessing ... that's guessing wrong!
Fluorescence tool measures changes
There is new dental technology available that can help eliminate the watching and guessing about unrestored teeth. The process is called laser caries detection, which uses fluorescence to determine the presence, absence, or extent of caries in unrestored teeth by measuring the characteristics (changes) of tooth tissue associated with bacteria. KaVo America's instrument is called DIAGNOdentRegistered. DIAGNOdent's objective is to improve the current techniques in caries detection. Doctors should understand why quantitive laser fluorescence should become the preferred technique, or at least a partner, in the early detection of primary carious lesions.
DIAGNOdent is a battery-operated unit consisting of a monitor and a solid-state laser in the shape of a probe. It is very light and can be easily moved from room to room. Therefore, one unit can service one to four operatories.
There are two interchangeable probe tips that are autoclavable. However, if they are to be used frequently, it is best to place a barrier (sleeve) over the tip, much like your intraoral camera wand. Tip A is for occlusal caries. Tip B is for smooth surface caries (facial/lingual). It must be noted that DIAGNOdent will not detect decay interproximally or under and around existing amalgam or composite restorations. However, it will be able to detect decay under a sealant.
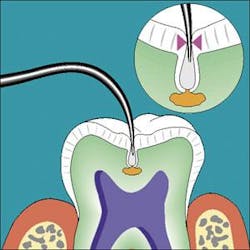
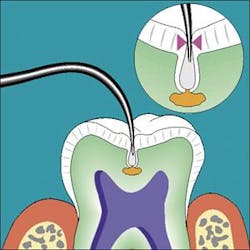
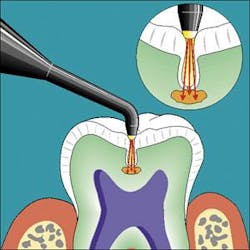
DIAGNOdent's use is simple. Prior to examination, dry the tooth thoroughly. The probe tip is gently placed against the tooth, enabling the laser beam to penetrate the surface and subsurface enamel. The tip may be rotated to accurately obtain measurements in all three dimensions. The measurements are digitally displayed on the monitor. The "moment" display gives the current real time value being measured as it is continuously changing. "Peak" display gives the maximum value recorded during any single tooth measurement.
The measurements are displayed digitally on the monitor while a sound is emitted, increasing in intensity as the extent of decay increases. Think of how impressive this is for patients or parents of children to be able to see and hear decay. And it is very easy to understand. For example, when I go to my physician and he takes my temperature, I watch the values being displayed digitally. If the thermometer displays a value higher than 98.6 degrees, I know it is not normal, so I am constantly watching it rise and hope that it stops at the appropriate value.
Healthy Outcomes Technology (www.healthyout comes.com) developed a Palm software for the DIAGNOdent called EviDent Lite to enable the doctor or hygienist to record and document the peak values of every tooth in the dentition. This is especially helpful in monitoring possible value changes between each patient visit. A baseline value can be recorded at an initial visit and compared to values at future visits to determine if decay has progressed. From a practice management standpoint, this is one more opportunity to provide a thorough and complete patient record.
What do the values mean? According to researchers, the following may be suggested. Values between 0-14 require no active care. Values between 15-20 require no active care but possibly preventive treatment only. Values between 21-30 require preventive treatment or active care, depending on the patient's caries risk. Values greater than 30 require active restorative treatment.
From observations in my private practice, these values are consistent with our findings as to whether preventive, active, or no treatment is required. In many instances, using routine DIAGNOdent examination, values less than 30 have been recorded without radiographic or clinical evidence of decay.
Restorative treatment was justified in these instances, while, prior to DIAGNOdent, we would have watched these teeth. Watch them do what? In every one of these cases decay existed, so we would have watched the decay process progress. Although we have no long-term studies, many sealants have been placed preventively when recorded values presented between 15 and 20. Clinical studies have demonstrated that in these cases, placing sealants will abort the decay process.
Therefore, we are no longer guessing and we are not guessing wrong. The result has been very impressive and reassuring with patients, especially parents of children and adolescents. They are comfortable and accept the high tech adjunctive diagnostic capability DIAGNOdent affords. They believe that diagnostically, everything that could be done was done, and they could see and hear it for themselves.
Charles D. Samaras, DMD, is the director of practice management at Tufts University School Of Dental Medicine. He maintains a practice specializing in esthetic and restorative dentistry in Lowell, Mass. Dr. Samaras may be reached by email at [email protected] or [email protected].