Chew on this
By Shirley Gutkowski
http://search.cdc.gov/search97cgi/s97is.dll?Collection=cdcall1&SortField=score&action=search&Filter=newsearch.hts&ResultTemplate=nsearchresult.hts&qbedoc=http%3A%2F%2Fwww%2Ecdc%2Egov%2Fnchs%2Fppt%2Fhp2000%2Fdisparitycharts%2Eppt&
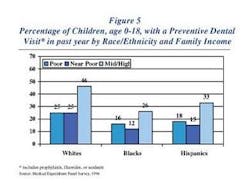
As you can see by the above Web address, I had a little difficulty coming up with the information in the accompanying graph. I found it at the Centers for Disease Control and Prevention site, with a couple of magic strokes of my fingers on the keyboard and about 60 minutes. I wanted to write this month about treating decay, and more importantly using everything we know to access those who have difficulty accessing us.
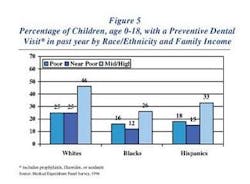
The graphic shows the difficulty people have accessing dental care in 1996. Today's numbers could be better or worse, or the same. The chart does not reflect the last visit, which may have been 13 months prior, or the next visit, which may be next week. The chart also shows the near- poor are having more difficulty than the poor. In fact, only 12 percent of the near-poor Blacks have had a preventive dental care visit in the last year. That's just over one in 10! Since we have some unknown variables, I think it is wise to just take the information at face value.
What if the other 78 percent called your office for an appointment tomorrow? Could you see them? How many more hygienists would be needed to provide preventive services to that many more people? The high school in our small city allowed nearly one-third of its student body to be truant every single day because they did not know where to put them all. What to do, what to do?
One way to help achieve the Healthy People 2010 oral health goal is for hygienists to do outreach. Within the guidelines of the law, hygienists of all educational backgrounds can go forth and educate.
Another way is to really teach our patient (read: students) one at a time, so that they can go and educate others in their sphere of influence.
The most fun trick to teach them is about gum. They've heard the brush and floss lecture, or you may not have a chance to get to that section of Lecture #35 since their body language says, "Back off, lady; my brain is on pause until the droning stops." The telltale glazed eyeballs, the metronome bobbing of the head and the sound, "uh huh" all are codes for get me the heck out of here! Lecture #35 is not going to penetrate. You've lost the patient to simple statistics before you've begun. Lecture #35 assures this patient a majority placement in that more than 70 percent of patients who don't come in even once a year for the duration of their time on the planet, and the pain that goes along with it.
Yeah, but gum? How is that helping? It'll be confusing for them, won't it? I submit that it's no more confusing than brushing twice a day. We just have to give our students a short list to choose from: xylitol gum or Recaldent™-containing gum. I had the rare opportunity to speak to the lead researcher of Recaldent, Dr. Eric Reynolds, during an international phone call to Australia this past summer. What a fantastic discovery.
Recaldent comes from the casein in milk. People from Wisconsin, New York, and California know what casein is. It's the part of milk that cheese makers use to make cheese. It is also the part of milk used to make Recaldent. Please note that there's no lactose. People who are lactose intolerant don't have to worry about using it, while those with allergies to milk can be sensitive to it.
Milk has the basics to rebuild acid-damaged enamel. The chemists and researchers in Australia have isolated the components to do that — calcium and phosphorous. These two elements are attracted to each other so strongly that they usually bond together before they get to the tooth and bond to it. The magic is that Recaldent contains amorphous calcium and phosphorous, which remain suspended until they can bond to the tooth.
Dr. Reynolds said that the best time to use Recaldent is right after a fluoride application. So, in the office is a good place to start. As you're giving your student a toothbrush and escorting them to the door, give them some Trident for Kids to chew. Since Recaldent and fluoride work in tandem there's no need to wait the 30 minutes. It is also best to use this ingredient right after brushing with fluoride toothpaste at home.
Recaldent enhances the effects of fluoride. Fluoride is dose-dependent on the calcium and phosphorus content of saliva, which are the exact components of Recaldent. The effect is additive. Whatever effect one gets with fluoride alone is added to the effect of Recaldent.
Some studies have shown that chewing for five minutes is long enough to get the total advantages. The benefits extend further than basic remineralization. If we stay on the track of the 70-plus percent of near poor people that don't get yearly preventive visits we have to realize that their general home care is less than what hygienists consider adequate. While poor doesn't equal poor health on an individual basis, statistically that's true. Poor does equal poor oral hygiene, statistically.
Some oral health care providers figure including adjuncts such as fluoride mouth wash, lozenges or gum isn't worth it if oral hygiene isn't impeccable. Their working theory is that if there's still plaque on the teeth, nothing works. Well, that's far from the truth. Even fluoride seeps through plaque, working with the lower pH to remineralize teeth. That is how fluoridated water works (CDC 2001). Recaldent also can make its way through the biofilm to remineralize enamel.
Acids produced by the oral biofilm seep between the enamel rods to create decay under the outer surface of enamel. Fluoride works on the surface, binding with the top layer of the tooth's enamel creating a less permeable layer of fluorapatite (JADA 2000). Once the constant assault of acid is lessened by plaque removal or dietary changes (elimination of soda, for example) this fluorapatite protects the underlying weakened enamel from future attacks. Recaldent supplies the amorphous calcium and phosphorous to build up the weakened enamel from the bottom. Healing lesions from the bottom-up eliminates the white spot, giving the enamel a translucency much the same as enamel that hasn't suffered the disfiguring effects of too much acid.
Professional application of Recaldent in the future will allow clinicians the ability to rebuild enamel in the office. In a procedure much like polishing, white spot lesions on a microscopic level will be filled in, built up, to where the patient will no longer have those bracket marks on their teeth. The hope is that this technology will be available to clinicians in less than five years.
So far, Recaldent is available in two of the Trident gums. One is more suited for adult taste buds, the other good for children. This technology is so important on so many levels. Residents of nursing homes benefit profoundly from chewing gums. Better ability to taste and chewing, a better feeling mouth, and better muscle tone are just some advantages to chewing sugar free gum. Patients who undergo radiation therapy of the head and neck also benefit greatly. The problem arises with the strong mint flavoring for those people. The gum can create a burning sensation. My hope is that a flavor-free gum or one with milder flavor can be developed for these groups.
Xylitol in any form — gum, lozenges, or crystals — inhibits metabolism of the major culprits of decay progression. It also helps to remineralize areas that have already broken down. The fun aspect of xylitol is that it is the preferred sugar of S. Mutans. It will let sucrose pass by as it waits anxiously for another shot of xylitol. It will starve in the process. Its environment will change to one that is incompatible to streptococcus life, due to the increased pH. The biofilm, while still apparent to the naked eye, is vastly less harmful as the malicious bacteria are fewer and fewer in number.
When given to mothers before their babies get teeth, xylitol decreases the number of decayed teeth dramatically in the children (JDH 2003). In a time when baby bottle decay is so insidious in the poor and near-poor populations, not teaching our patients about the benefits of xylitol is reckless. We can do more. Gum containing xylitol is readily available. It's easy to access, easy to chew, and curative.
Once access to preventive care is achieved, oral health care providers must make the biggest impact possible with the least amount of nagging. Chewing sugarless gum is a perfect adjunct to teach this group. The action of chewing sugarless gum has been proven to enhance remineralization in application as infrequent as 15 minutes after each meal. This level of rebuilding has proven to be doubled with the use of Recaldent effectively giving double the bang of the buck.
Fear of giving the wrong message must be overridden by knowledge that giving an education to the one in the chair will increase the chance that something will click.
I'm forced again to point to commercials. If you turned on your television tonight and heard "Where's the Beef?" one more time you'd shoot out the screen. If you turned on the radio and heard I Wanna Hold Your Hand again, you'd probably cry. Marketers know that variety is the ticket to holding the public's interest in a topic. Coming to patients/clients with Lecture #35 again is doing them and the profession a disservice.
References
• Recommendations for using Fluoride to Prevent and Control Dental Caries in the United States http://www.cdc.mmwr/preview/mmwrhtml/rr501a1.htm
• Featherstone J. The Science and Practice of Caries Prevention JADA July 2000 vol 131 887-899
• Peldyak J. Xylitol for Caries Prevention. Journal of Dent Hyg. Vol 76 no IV 276-283
Shirley Gutkowski, RDH, BSDH, has been a full time practicing dental hygienist in Madison, Wis., since 1986. Ms. Gutkowski is published in print and on Internet sites, and speaks to groups through Cross Links Presentations. She can be contacted at [email protected].