Finding the right dry mouth fit

Patti DiGangi, BS, RDH
Dental professionals, particularly hygienists, bond with patients quickly—often during the first visit. That is what happened with Connie and me. She was a health-aware person, diagnosed with multiple sclerosis 25 years before her first visit. Connie shared that her dry mouth was one of her biggest challenges. She said sometimes she didn’t have enough saliva to chew her food. By the end of the visit, she took my hands and said, “God is taking my legs—can you help me keep my teeth?” What an honor! What a challenge.
Based on her risk and to maintain her quality of life, Connie saw me every two to three months. At every visit there was a complete evaluation and discussion of her dry mouth needs. Why? Because every time Connie came into the office, she was different than she had been at the last visit . . . just like all of our patients.

© Photomall - Dreamstime.com
A dry mouth condition is not static. Evaluation is needed at every visit to create the best comfort and preventive care plan. There are many arrows in the quiver of product choices. Care must be taken to recommend products that are safe, effective, and the right fit for each individual.
At least 30% of your patients are afflicted
Many of us take saliva for granted, but when this natural function is diminished or stops, the quality of life can drastically change. Connie described her dryness as her tongue and palate feeling like halves of Velcro.
Dry mouth is a very common problem and is far more prevalent than many clinicians think. Reported rates of dry mouth vary with age and geographic areas. Though there are inconsistencies between studies, it is estimated that dry mouth affects up to 64% of the population.1 Using a conservative estimate, if you are not treating at least 30% of your patients for dry mouth, you could be underdiagnosing and undertreating this condition.
The words xerostomia and hyposalivation are often used interchangeably. This can lead to errors in thinking and treatments. Xerostomia can be a symptom of salivary gland hypofunction (SGH).2 A dry mouth feeling (xerostomia) can occur with no decrease in salivary flow. They are not interchangeable terms.
Even with SGH, salivary flow can be decreased as much as half before a person might realize it. Patients don’t know they have to manage their symptoms. They have become accustomed to the feeling, do not know options, or create coping behaviors that sometimes worsen the consequences of the condition.
Early detection and accurate determination of the specific condition and/or contributing factors can be key to helping the patient. There are no one-size-fits-all solutions.
Saliva diagnostics
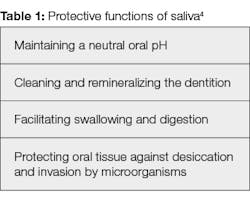
The many inorganic and organic compounds in saliva have been described as a “mirror of the body’s health.”3 Table 1 lists a few of the important functions from an oral perspective. Oral care is the purview of the dental profession; this is not limited to only what happens in the mouth. The Centers for Medicare and Medicaid Services recently recognized the importance of oral care when it redefined the term
“physician” to include “doctors of dental surgery of dental medicine.”5
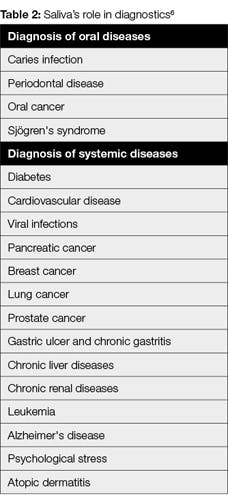
Dental professionals have the opportunity to play a role in the detection of systemic diseases. Table 2 shows lists of the diseases that can be detected with saliva. There are many advantages of using saliva as a diagnostic fluid including that it is “simple to collect, convenient to store, essentially noninvasive, and contains high-quality DNA.”6 Anyone who has watched any of the multiple television programs about crime scenes has heard of the power of DNA in saliva. Bottom line: saliva is important.
Symptoms of dry mouth
Dry mouth symptoms vary from person to person and differently for the same individual based on his or her changing health status. Some are perceived by the patient; others may not be.
• Bad breath
• A sticky, dry, or sore mouth
• Cracking at the corners of the mouth
• A red and parched mouth
• Blisters and mouth ulcers
• A pebbled look to the tongue
• Difficulty eating dry or spicy foods
• Difficulty speaking
• Thirsty at night
• Waking up with a dry mouth at night
Drinking more water is not a solution to dry mouth. Though saliva is 99% water, the 1% contains the most amazing and important ingredients—secretory proteins, immunoglobulins, electrolytes, antibodies and wound healing components. Many of our patients are deprived of this healthy, healing fluid. It is our duty to treat this high-risk condition.
Chairside screening
Before disease occurs, there is health with risk for disease. This is well understood with heart disease. Many people take blood pressure and cholesterol medication to reduce the risk of a heart attack. A side effect of many of these medications is dry mouth.
Polypharmacy, defined as taking more than three medications, is a major contributing factor to dry mouth. Many forms do not have the space needed for a complete listing of medications. Patients may not list all of their medications if they do not understand the effect medications can have on their oral condition.
Risk assessment starts with an oral review of the current health status. It can seem efficient to hand someone a form with boxes to check, but many patients may not be able to read or understand the health form.
A news story published 20 years ago told of a retired school teacher admitting he was illiterate until the age of 48.7 Unfortunately, literacy is still a real issue. According to a study conducted in late April 2015 by the US Department of Education and the National Institute of Literacy, 32 million adults in the United States can’t read above a fifth-grade level and 19% of high school graduates can’t read.8 Even if your patient is literate, it is quite possible that he or she didn’t understand many of the questions. An oral review with the patient is key.
A simple assessment starts with these questions: Does the amount of saliva in your mouth seem to be too little? Does your mouth feel dry when eating a meal? Do you sip liquids to aid in swallowing dry food? Do you have difficulty swallowing?2 A positive response is an important indication for further assessment.
Oral biologist and dental hygiene educatorMargaret J. Fehrenbach, MS, RDH, developed a validated tool for screening, assessment, and management of hyposalivation with xerostomia. This screening tool is designed to be convenient, efficient, and accurate by using checkboxes to determine treatment steps.9 You can watch a video about this tool and get a copy at bit.ly/fehrenbach.
Chairside tests
Dental caries is a biofilm-mediated, pH-specific disease. It is not a hole in a tooth. The hole in the tooth (the decay) is an outcome of a disease process. The mouth is a natural ecosystem. To stay healthy, it needs to maintain a proper balance. Enamel breakdown starts when oral pH falls below 5.5. An important function of saliva is maintaining a neutral oral pH. When salivary flow is reduced, its buffering effect is also reduced.
A simple and unique disclosing product, GC Tri Plaque ID Gel (GC America) gives important risk information. A pH value cannot be seen with the naked eye. There is no other disclosing product that gives an indication of pH.
As with many disclosing products, newer, thin deposits of biofilm will stain pink/red. Thick deposits of biofilm will stain blue/purple. Areas that are light blue indicate acid production. The biofilm has a of pH 4.5 or lower. Without adequate saliva, damage occurs. The provider needs to consider further testing.
Saliva-Check Buffer (GC America) is a saliva-testing assessment tool. This product plays a significant role in maintaining oral health. It identifies, measures, and assesses the patient’s saliva condition. It is helpful for testing hydration, salivary consistency, resting saliva pH, stimulated saliva flow, stimulated saliva pH, and salivary buffering capacity. Saliva-Check Buffer provides important information to assist in preventive treatment planning and proper selection of dental materials.
The greatest value for both of these products is that patients and providers can visualize what is not normally visible. Our tradition has been to treat and take care of what we, as the providers, see as the problem. Unless the patient sees and owns the problem, our treatment will only resolve the issues temporarily. The chronicity of oral dryness causes the damage. Short-term care only provides short-term resolution.
Product pH levels
Risk factors are numerous and are either modifiable or nonmodifiable. Behavior modification is the patient’s choice. Connie could not modify her multiple sclerosis or her medication regimen. Palliative care included oral patches, rinses, lozenges, toothpastes, sprays, gels, and chewing gums.
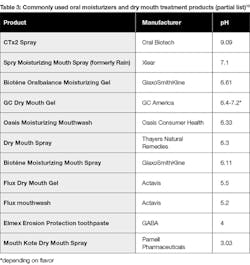
Before recommending any of the products, I recommend health-care providers read the important article “Acidic oral moisturizer with pH below 6.7 may be harmful to teeth depending on formulation.” University researchers Delgado and Olafsson published this article through the National Institutes of Health reporting that to be safe, oral moisturizers should have an acidity level of 6.7 pH or higher. Further, oral moisturizers with a pH below 5.5 are dangerous, citing one with a pH of 3.03.9 See Table 3.
Product choices
There are numerous quality choices for dry mouth care available. For example, GC Dry Mouth Gel (GC America) with a neutral pH is designed to ease the symptoms of dry mouth for patients who may be suffering from impaired production of saliva due to medications, radiation treatment, or diseases that can damage the salivary glands. It provides a protective coating for teeth and oral tissue.
MI Paste and MI Paste Plus (GC America) are the only products for professional use containing the active ingredient Recaldent, a special milk-derived protein that has a unique ability to release bioavailable calcium to tooth surfaces and oral tissues. When it comes to maintaining a healthy smile, these key ingredients can make a big difference in overall health. MI Paste Plus offers the same benefits of MI Paste but is enhanced with fluoride (900 ppm).
The newest addition to the MI Paste line is a two-in-one application. MI Paste One can be a replacement for current toothpaste. It gives the same power of MI Paste Plus, but in a single application and with more fluoride (1,100 ppm). MI Paste One is designed to be gentle to the tooth but with high cleaning efficacy, with a low relative dentin abrasivity (RDA) value of 64. Many patients with dry mouth are particularly susceptible to mucosal irritation, so MI Paste One is sodium lauryl sulfate free. Instead, it contains a milder surfactant; the mild foaming helps to reduce the discomfort after brushing.
Making a difference
Some patients, like Connie, find that using a combination of GC Dry Mouth Gel and MI Paste gives them comfort. Before going to sleep, Connie dabbed some MI Paste on her tongue. Rather than keep water by her bedside, she kept MI Paste. If she awoke during the night, she dabbed on more.
Connie’s health was not static. At each two-to-three month visit, we changed something—added, subtracted, and evolved how she might use the arrows in the quiver. Unfortunately, we lost Connie in late 2016, but what an honor it was to know her and help maintain her quality of life.
References
1. Owens J, Gibson BJ, Periyakaruppiah K, Baker SR, Robinson PG. Impairment effects, disability and dry mouth: Exploring the public and private dimensions. Health (London). 2014;18(5):509-25. doi: 10.1177/1363459313516137.
2. ADA Council of Scientific Affairs. Managing xerostomia and salivary gland hypofunction. https://www.ada.org/~/media/ADA/Science%20and%20Research/Files/CSA_Managing_Xerostomia.pdf?la=en. Published February 2015.
3. Greabu M, Battino M, Mohora M, et al. Saliva—a diagnostic window to the body, both in health and disease. J Med Life. 2009;2(2):124-132.
4. Oral health topics: Salivary diagnostics. American Dental Association website. https://www.ada.org/en/member-center/oral-health-topics/salivary-diagnostics. Updated August 28, 2018.
5. Centers for Medicare and Medicaid Services. MMA-Private Contract Manual Change to Include Dentists, Podiatrists, and Optometrists in the Definition/List of Physicians Who Can Opt Out of Medicare. https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/downloads/mm3016.pdf. MLN Matters Number: MM3. Updated April 22, 2013.
6. Zhang CZ, Cheng XQ, Li JY, Zhang P, Yi P, Xu X, Zhou XD. Saliva in the diagnosis of diseases. Int J Oral Sci. 2016;8(3):133-7. doi: 10.1038/ijos.2016.38.
7. Our story. John Corcoran Foundation website. https://www.johncorcoranfoundation.org/.
8. About us. Literacy Inc website. http://literacyinc.com/about-us/.
9. Fehrenbach MJ. ADHA Hyposalivation with Xerostomia Screening Tool Project. Poster presented at: ADHA CLL 2013. http://jdh.adha.org/content/jdenthyg/87/6/378.full.pdf.
10. Delgado AJ, Olafsson VG. Acidic oral moisturizers with pH below 6.7 may be harmful to teeth depending on formulation: a short report. Clin Cosmet Investig Dent. 20017;9:81-83.
Patti DiGangi, BS, RDH, is an international speaker who is passionate about prevention and working with dental professionals to improve practice profitability. Patti is the author of the DentalCodeology book series for busy dental professionals. She recently published DentalCodeology: Critical Decisions Workbook: Teledentistry Pathway to Prosperity, coauthored by Cindy Purdy, RDH. Patti also holds publishing and speaking licenses with the American Dental Association for CDT and SNODENT.