Ergonomics: • Pain Management vs. Pain Elimination •


Harold L. Meador, DDS, is a clinical associate professor in the Department of Periodontics at The University of Texas Health Science Center at San Antonio, Dental School and is a senior research fellow in the Center for Health Economics and Policy. Dr. Meador had a general dentistry practice for eight years and maintained a practice limited to periodontics in San Antonio for 36 years. In the past, Dr. Meador has lectured and published articles on periodontics and dental insurance. Since 1985, he has studied, conducted clinical research, published articles, and presented programs on instrumentation techniques, focusing on the ergonomic and orthopedic principles that impact the hygienist.
The longevity of a pain-free dental career is based on proper ergonomics for each dental team member. It’s been said, “It’s not a matter of if you will have pain during your dental career, but when.” If you already experience pain, why would you just want to manage it if there was a possibility you could totally eliminate it?
During 25 years of working with thousands of hygienists, The JP Institute understands that dental hygienists’ duties can result in occupational pain which can often be debilitating. The Institute has researched many possible solutions to this problem, such as acupuncture, different styles of physical therapy and reflexology that may assist with pain management. While these are great resources to manage pain and provide healing, an even better solution is to avoid pain altogether. Is there a way for the dental hygienist to do this?
The first revolutionary prospect of pain reduction for the dental hygienist came with the technology of microultrasonic therapy. The clinical benefits were exciting, and the mere thought of reducing time spent on repetitive motions, as well as the amount of strength needed to properly root plane teeth, made most hygienists jump for joy! We were excited to think that pain related to the services we provide could be eliminated.
Unfortunately, complete eradication of pain did not occur. What other options could there be? Throughout The JP Institute’s history of working with hygienists in numerous clinical capacities, many professional colleagues told us about how Harold Meador, DDS, BSD, a retired periodontist in San Antonio, produced amazing results for pain prevention and elimination for the dental team. Dr. Meador is the founder of the Wedgewood Periodontal Group in San Antonio, and he has been a clinical associate professor in the Department of Periodontics, UTHSCA, since 1978. His research during the last 20 years has focused on occupational pain. Recently, we had the opportunity to talk with Dr. Meador regarding his work on pain prevention and elimination for the dental team.
Peggy Sprague, RDH - Dr. Meador, why did you become interested in pain prevention/elimination for the dental team?
Harold L. Meador, DDS - My personal interest in coping with pain began when I experienced career-threatening symptoms as a young periodontist. Neuromusculoskeletal pain is common in many occupations, such as dental hygiene, that involve repetitive motions. It has become a matter of concern because of its impact on work loss and job security. Among dental hygienists, it is actually back problems that occur more frequently than problems of the wrist and hand, but painful syndromes of the upper extremity have been documented frequently in orthopedic journals. Carpel tunnel syndrome (CTS) has received the most attention in literature and research. CTS is probably the most dreaded condition of all nerve entrapment syndromes of the upper extremity.
PS - Would you please describe your theory and how it is different from other approaches?
HM - Suggestions for pain alleviation are usually limited to improving posture and biomedical interventions such as strengthening exercises. A different approach is to look at how neuromuscular pain could be related to currently accepted instrumentation techniques, and how new instrumentation theories and principles may help correct the problem. I have also become aware of a new dimension in this issue. Due to the long-standing history of pain with the dental team, it has been accepted as inevitable. Many hygienists suffer needlessly because they have no hope. My message is simple: There is hope. In reality no one bats 1,000; however, our track record is very respectable.
Based on evidential research of orthopedic literature, many years of clinical observation, and the positive feedback I have received from continuing-education classes I have taught since 1985, I believe that there is a cause/effect relationship between instrumentation technique and neuromusculoskeletal pain. It is my opinion, with concurrence from orthopedists, that exacerbations of the neuromusculoskeletal problems in dental hygienists are likely to occur for two reasons: violations of the neutral position of joints and excessive use of a few small muscles.
PS - Could you describe your approach to teaching pain elimination?
HM - My course consists of a lecture which establishes ergonomic and orthopedic principles, followed by a hands-on, one-on-one session using a mannequin placed on a dental chair, which is essential to create the skill transfer of work motions.
PS - What do you consider to be the most crucial point in creating this skill transfer?
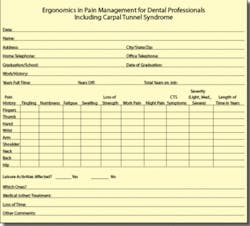
HM - I’m glad you asked that. The basis of my teaching starts with establishing the pain profile of every person in the class. I believe that a person learns best when his/her individual needs are addressed. This is accomplished with the “Ergonomics in Pain Management for Dental Professionals” questionnaire (see chart), which is a valuable tool that helps individuals see how these principles apply to them. It has been used for 14 years.
PS - Could you tell us about the techniques you use to prevent and eliminate pain for the dental hygienist?
HM - In 1960 I developed and taught a full-arm motion technique. After years of research and refinement, it was named the BioCentric Technique (BT), which is based on a three-part strategy for dealing with the fundamental causes of occupational pain: Violating the neutral position of joints; exhausting vital muscle groups; and working in an ergonomically negative work environment.
The first strategy involves keeping the joints in a neutral position as much as possible during instrumentation. This includes the shoulder, elbow, and wrist joints. The next strategy entails maintaining flexibility for shifting the workload to different muscle groups. Transferring the workload to various muscle groups allows the operator to work indefinitely without fatigue, because each muscle group has fresh energy to continue the task. This is called the work/rest mode, which includes combinations of instrument grasp, finger rests, chair position, and power strokes. BT employs three instrument grasps. The standard/modified grasp has been used for many years, but it was imperative to add two more instrument grasps: conventional and extended. In the conventional grasp, the instrument is held between the pads of the first two fingers at a 90-degree angle to the long axis of the forearm (LAOF), whereas the extended grasp uses the pad of the middle finger and the “notch” at the base of the forefinger, with the instrument held at a 30-degree angle to the LAOF. The ideal grasp is within this 60-degree zone between the two positions, allowing for a great deal of flexibility for the operator. The third strategy involves establishing an ergonomically friendly work environment, because over time it became apparent to me that it was impossible to establish proper posture and work motions in the average dental operatory.
PS - Why is the position of the hand important?
HM - Current positioning methods compromise both the elbow and wrist joints. BT places the back of the hand in a vertical plane with the palm to the side, which is the neutral position for the rotational motion of the elbow. As to the fingers, in the past external finger rests were often discouraged. BT endorses both internal and external finger rests.
PS - What do you suggest for chair positioning?
HM - I suggest the 7, 9, and 12 o’clock chair positions. The 7 o’clock position places the operator in front of the patient and as close to the chair as possible. In the 9 o’clock position, the operator is even with the patient’s head, and in the 12 o’clock position, the operator is above the patient’s head. It is important to constantly use different chair positions just to keep the body geometry flexible.
PS - Based on your work with hygienists over the years, what have you observed about power strokes? How do they relate to the BioCentric Technique?
HM - Most dental hygienists employ two basic power strokes - one a rotary motion of the wrist and arm, and the other a waving motion of the wrist. Both entail wrist movement that violates the neutrality of the joints. This is a wrist activation instrumentation system. The BioCentric Technique is a full-arm motion technique. The goal of power strokes - including rocking, pumping, swing, and push-pull - is to use the large and durable muscle groups of the arm and shoulder rather than those of the forearm and hand only. This is the work/rest mode that I mentioned earlier.
PS - Very intriguing. Dr. Meador, could you summarize the features of the BioCentric Technique?
HM - Absolutely. The system is based on sound ergonomic and orthopedic principles and centers on using the pain profile of individuals to aid them in dealing with the three main dynamics of occupational pain. First, the core of the BioCentric Technique is to prevent the violation of the neutral positions of the joints with proper posture and by keeping the joints in neutral. Secondly, the work/rest mode is designed to keep fresh muscle groups in use, thus avoiding exhaustion of vital muscle groups that results in fatigue. This means having multiple options for instrument grasps, finger rests, chair positions, and power strokes. Finally, creating an ergonomically friendly work environment involves taking a close look at the floor plan, instrument locations, and equipment in the operatory.
BioCentric Seminars are the direct result of helping several hygienists with their work-related pain. The positive feedback we have received regarding improved self-image and quality of life is the sustaining force and the reason for our efforts.
PS - Dr. Meador, thank you for your time. On behalf of dental hygienists everywhere, thank you for the significant contributions you have made to the likelihood that we will experience long, happy, pain-free careers!
HM - It has been my pleasure. For further information on ergonomics and pain prevention/elimination, please visit my Web site at www.biocentric.uthscsa.edu (The site is currently in the process of being updated). For those who are interested in our pain questionnaire and the pain questionnaire analysis (the analysis contains helpful suggestions), contact The JP Institute at (800) 946-4944, or email [email protected].
The JP Institute commends Dr. Meador for his pioneering efforts in ergonomics, which continue to have a positive impact on individual dental team members and the dental practice itself. In the same spirit as Dr. Meador’s contributions The JP Institute utilizes the latest evidence-based science to coach dental teams in advanced clinical protocols and technologies to achieve clinical excellence and exceptional profit margins. RDH