Tooth erosion Q&A

Tooth erosion is an ongoing (and seemingly growing) problem for patients today. As providers of care, it’s critical that we remain current on this topic. Let’s look at the causes of erosion (including cultural ones), the science behind it, and some novel treatments. We’ve broken everything down into six questions to help you wrap your head around the information. So, without further ado, let’s get started with our first Q&A.
Question 1: What do Beyoncé’s Master Cleanse lemonade diet, Kourtney Kardashian’s “detox water,” or any of a dozen other celebrity green juice and smoothie recipes have in common?
Answer: From the dental point of view, we think of all that lost enamel! Lemons and limes contain citric acid, which has a pH of 2 to 3. This means that it’s 10,000 to 100,000 times more acidic than water. As shown in Figure 1, long-term sipping of acidic beverages, although aimed at health, has a massive impact on teeth.

It may be the fad of following celebrity diet and exercise regimes that has resulted in tooth erosion seemingly becoming more common, particularly in the younger generations. Much of this erosion is thought to be due to the consumption of acidic beverages.1 Erosion can occur with healthy fruit juices and smoothies, just as it can with sugar-laden sodas. Young adults can drink large amounts of these beverages. One study reported 31 ounces consumed per day among children aged 13 to 18 in the United States.2 In a similar survey conducted in the United Kingdom, 64% of 14-year-olds showed erosion in their permanent teeth, with 13% showing deep erosion or dentin involvement.3 Studies comparing children’s experiences in the United States and the United Kingdom show similar rates in both countries.4
When we see a new patient, how can we determine if this is a problem that occurred in the past or is an ongoing one? One predictor for progression of tooth erosion is having four or more intakes of dietary acid per day. Other predictors include saliva with a low buffering capacity or use of a hard toothbrush.5 These predictors can give us inspiration as to the strategies needed to break the erosion cycle.
We also need to consider that tooth erosion isn’t caused by extrinsic sources alone. Acid reflux (GERD) and bulimia can be sources of intrinsic acid erosion, and they can be just as devastating. The appearance of intrinsic acid damage usually shows with a different pattern of tooth surface loss. This pattern is essential to recognize for diagnosis, prevention, and treatment. Extrinsic erosion will typically affect the occlusal and facial surfaces of upper and lower teeth, whereas intrinsic acid will more likely affect the palatal surfaces of the maxillary anterior teeth in addition to the lower molars. The effects of erosion can be worsened by wear from abrasion and attrition.
As an example, Figure 2 shows images of a 20-year-old man with a complicated health history and a daily intake of three to four cans of soda (Mountain Dew). He denied vomiting or an eating disorder. However, there was the potential that the carbonated drink intake induced reflux. The man’s erosion pattern was typical of intrinsic acid damage to the palatal of the upper teeth and lower posterior teeth.



Question 2: Is fruit juice more harmful to teeth than soda?
Answer: This is a tricky question, as there are large variations in the recipes and additives of both juices and sodas. It is well recognized that sugar in sodas is harmful to teeth and our health as a whole. However, fruit juices and smoothies can also have high sugar content, as the fibrous cells of the plant-based ingredients are damaged in the processing of the drinks, which releases their natural sugars. Remember: cariogenic bacteria do not discriminate between natural and refined sugars!
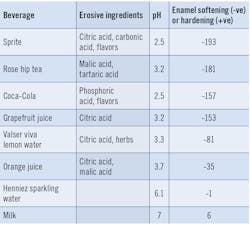
If we are concerned purely with erosion, then the acidity in sodas such as Coca-Cola originates from phosphoric acid, whereas citrus fruit contains citric acid and malic acid. With tooth erosion, it is easy to think of the effects of a strong acid versus a weak acid, and consider that one will be more damaging than the other. However, there are a number of factors that affect the amount of dissolution of a tooth. A better measurement of harm may be the effect of enamel softening to show the erosive potential of a food or drink.6 As you can see in Table 1, some fruit juices can be as damaging as carbonated drinks. Somewhat surprising to many patients is the fact that sparkling water is not damaging to teeth until the acidic flavors have been added.
Question 3: Is the elementary school experiment of dissolving baby teeth in soda realistic?
Answer: It’s not just the acidity (pH) of soda that’s important in this experiment, and here’s why. Tooth erosion differs from caries, as it involves the surface removal of tooth substance not associated with plaque. There is a difference in how acids affect enamel and dentin because of these substances’ mineral makeup. In a real-life scenario, there is biofilm (acquired pellicle) covering the surface of the tooth. For erosion to occur, acid needs to diffuse through the protective biofilm and then dissolve the enamel prisms, softening the outer surface of the enamel. The enamel is then more susceptible to abrasion and attrition, such as with toothbrushing.7
Where there has been gingival recession, the exposed dentin can suffer from erosion too. Calcium and phosphate ions are stripped out by acid, which exposes the organic matrix of collagen. The collagen scaffold can be beneficial and trap the released calcium, which slows more demineralization. The network of collagen also forms a barrier to dentin loss by attrition or abrasion, but the effect of salivary enzymes can mean this protective layer is ultimately lost, and further progression can occur.7 The appearance of tooth loss due to the combination of erosion with abrasion in enamel and dentin can be seen in Figure 3.

So what is the difference between our mouths and the school experiment? In the classroom, the tooth is often left in one glass of Coca-Cola, whereas in our mouths, the beverage is usually swallowed quickly, flushing away the acid and allowing the saliva to dilute and neutralize the acid by its buffering effect. Unfortunately, we often observe people sipping on sodas over a long period, constantly replenishing a new supply of acid, and this can be even worse if the drink is swished around the teeth. As we may remember from our high school chemistry lessons, increasing temperatures often increases reactivity, and this is the case for hot beverages such as fruit teas, which show greater enamel stripping effects than iced tea.
Question 5: What should you recommend to Beyoncé when she visits your office?
Answer: Nothing is as good as keeping your natural teeth. But if erosion occurs, there are solutions, as shown in Figure 4.

Erosion can cause esthetic compromises to teeth with the loss of surface texture, thinning, chipping of edges, cupping on posterior teeth, and exposure of the dentin, which leads to sensitivity. When this is severe enough, we need to restore teeth, which costs substantial time and money for long-term replacements. Therefore, prevention is the key!
The first step is to identify the problem. Discuss with the patient what might be the origin of the erosion. Recording the extent of tooth surface loss by making dental casts, taking photos, and performing intraoral scans can be very useful to monitor the condition if it is progressive.
Reflux can be “silent,” so evidence of erosion caused by intrinsic acid without the patient having a history that identifies the cause may warrant a referral to his or her medical practitioner. If the origin of erosion is likely from extrinsic sources, then dietary advice is essential, such as with an information sheet tailored to the patient. Asking the patient to complete a four-day diary of food and beverage intake—which includes times and ideally occurs over two workdays and two nonworking days—will allow an assessment and advice on diet alterations.
Dental hygienists are typically great communicators. With dietary knowledge from the patient, hygienists can manage changes in receptive individuals.8 However, in a study in Oregon, only 53% of hygienists provided any dietary advice to patients.9 It is crucial that dental professionals are confident with nutritional advice and understand models of behavioral change, such as the transtheoretical model, to improve oral hygiene and nutritional outcomes.10 Alternative sources of information can be provided to patients from useful resources, including mouthhealthy.org and choosemyplate.gov.
Avoidance of slowly sipping on drinks or swishing drinks around the mouth is recommended. There is some research to suggest that using a straw to avoid contact with the front teeth is helpful. However, it is questionable whether it is feasible to position the straw in such a way to enjoy a beverage and avoid tooth damage. After all, despite all the information in this article, it is important to enjoy life too!
Individuals who suffer from dry mouth have reduced salivary protection by buffering and dilution. Patients with dry mouth may use salivary stimulants, and some of these can be acidic to mimic citrus fruits. Since citric acid has potential to erode the teeth, care is warranted in these high-risk patients.
Toothbrushing can increase the risk of attrition following an erosive challenge. We often recommend waiting an hour after an acidic challenge before brushing teeth, but studies have shown the enamel is still susceptible even after this time.7 In addition, the toothbrush type and brushing action has been shown to be more important in erosive tooth wear than waiting the hour.7 Using topical applications of Tooth Mousse (GC Corporation) can be beneficial in neutralizing acids and tooth sensitivity, as it contains a bioactive form of calcium phosphate. Care is required with some mouth rinses such as Listerine (pH 3.6), as this has been shown to cause significant erosive potential.11 Stannous fluoride mouth rinses are recommended following acidic challenges, particularly in patients with dry mouth or low buffering capacity of the saliva.5
Science is advancing in an attempt to neutralize acid damage through more patient-friendly products. An example is a product developed by one of the co-authors of this article, Michael Heffernan, BDS, called Dr. Heff’s Remarkable Mints (Dr. Heff’s Products Ltd.). This product contains a formulation of xylitol, green tea polyphenols, and calcium phosphate, and was designed to neutralize acid for patients on the go. The University of Illinois at Chicago College of Dentistry tested the product and found that remineralization in an erosive challenge was better achieved than with xylitol alone.12,13 In vivo studies showed rapid neutralization of acid even in thick plaque, with results comparable to sugar-free chewing gum but without the downsides.
Question 6: Can I create a great tasting, nonerosive detox water?
Answer: Our philosophy is that if we identify a problem, we should try to find a solution. If you want a rehydrating, nonerosive solution after your workout, we offer the following recipe:
Add three to four drops of lemon essential oil into a glass of water and pour into an ice cube tray to create flavored ice cubes. Lemon essential oil gives the “zing” without any acidity, as essential oils have neutral pHs.
Add sliced cucumber, ginger, a cup of gunpowder green tea that has been brewed and allowed to cool, and fresh mint to a jug of water. In a glass, pour over the flavored ice cubes.
This solution is truly beneficial and causes no erosion!
Conclusion
We all enjoy food and beverages that are acidic, but modern diets can be more damaging, particularly because of peer pressure and media influencers. In this article, we described a rational approach to identifying causes of tooth erosion and positive approaches to changing harmful habits.
Editor's note: This article was originally published in 2020 and has been updated as of May of 2025.
References
- Nunn JH, Gordon PH, Morris AJ, Pine CM, Walker A. Dental erosion—changing prevalence? A review of British National childrens’ surveys. Int J of Paediatr Dent. 2003;13(2):98-105.
- Jacobson MF. Liquid Candy. 2nd Ed. Washington, DC: Center for Science in the Public Interest; 2005.
- Dugmore CR, Rock WP. The progression of tooth erosion in a cohort of adolescents of mixed ethnicity. Int J of Paediatr Dent. 2003;13(5):295-303.
- Deery C, Wagner ML, Longbottom C, Simon R, Nugent ZJ. The prevalence of dental erosion in a United States and United Kingdom sample of adolescents. Pediatr Dent. 2000;22(6):505-510.
- Lussi A, Ganss C. Erosive tooth wear. Monogr Oral Sci. 2014;25:220-229. doi:10.1159/000360612
- Lussi A, Megert B, Shellis RP, Wang X. Analysis of the erosive effect of different dietary substances and medications. Brit J Nutr. 2012;107(2):252-262.
- Lussi A, Ganss C: Erosive tooth wear. Monogr Oral Sci. 2014;25:215-219. doi:10.1159/000360379
- Harris R, Gamboa A, Dailey Y, Ashcroft A. One-to-one dietary interventions undertaken in a dental setting to change dietary behaviour. Cochrane Database Syst Rev. 2012;3. doi: 10.1002/14651858.CD006540.pub2
- Levy TA, Raab CA. A study of the dietary counseling practices among Oregon dental hygienists. J of Dent Hyg. 1993;67(2):93-100.
- Wade KJ, Coates DE, Gauld RD, Livingstone V, Cullinan MP. Oral hygiene behaviors and readiness to change using the tanstheoretical model (TTM). N Z Dent J. 2013;109(2):64-68.
- Pontefract H, Hughes J, Kemp K, Yates R, Newcombe RG, Addy M. The erosive effects of some mouthrinses on enamel. A study in situ. J Clin Periodontol. 2001;28(4):319-324.
- Zamperini CA, Bedran-Russo AK. Remineralization potential of mints containing bioactive agents in artificially induced root caries. Caries Res. 2018;52(4):331-338.
- Padron AC, Zamperini CA, Bedran-Russo AK. In vitro anti-erosion property of a mint containing (−)-epigallocatechin-3-gallate in root surfaces. Department of Restorative Dentistry, UIC College of Dentistry unpublished data from research project. 2016.
About the Author

Michael Heffernan, BDS, MS
Michael Heffernan, BDS, MS, graduated from Guy’s Hospital and completed his master’s degree in prosthodontics at the University of Iowa. His research won the John J. Sharry Research Prize from the American College of Prosthodontists. Dr. Heffernan works clinically as a specialist prosthodontist. He has lectured internationally on implant dentistry and created Dr. Heff’s Remarkable Mints in 2014.

Rochelle Fodi, RDH
Rochelle Fodi, RDH, has practiced in a periodontal specialty setting for 40 years. She is licensed in Pennsylvania to administer anesthesia as a public health practitioner and as an emergency medical technician. Fodi has also practiced in Maine and South Carolina. She is a former clinical instructor at Northampton Community College.