When we get it wrong: Coping with misdiagnosis, stress, and building resilience through empathy
Key Highlights
- Missed oral pathology—especially lesions such as erythroplakia, leukoplakia, and early oral squamous cell carcinoma—often occurs not from lack of knowledge, but from gaps in documentation, follow-up, and time pressure in clinical practice.
- Diagnostic misses can carry a significant emotional burden for clinicians, with many experiencing second victim syndrome, including guilt, anxiety, and loss of confidence after adverse patient outcomes.
- Building resilience through clinical systems, mindful presence during exams, and self-compassion helps dental professionals learn from missed findings while maintaining strong patient care and professional well-being.

In the world of clinical care, precision is sacred. We are trained to spot subtleties, to diagnose with confidence, to know. Yet every experienced dental professional—hygienist, dentist, and assistant—carries this quiet truth: sometimes, we get it wrong.
Misdiagnosis happens. Suspicious lesions are overlooked. Symptoms are misread. Patients are misheard. And in oral pathology, where the margin between a benign finding and a life-altering diagnosis can be razor-thin, the stakes feel painfully high.
But what if we could approach these moments differently? What if the miss wasn’t a fracture in our identity, but a call to deepen our clinical eye?
This article explores the emotional and clinical weight of missed oral pathology, the lesions we most often misread, and how to build the kind of resilience that makes us better clinicians without destroying us in the process.
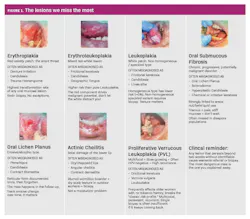
The lesions we miss most, and why it matters
Not all misses are created equal. Some carry more weight than others, and in oral pathology, the ones that cost us the most are often the ones hiding in plain sight (figure 1).1,2
Oral squamous cell carcinoma (OSCC) is the one that keeps clinicians up at night, and for good reason. Early-stage lesions often present as seemingly harmless findings: a white patch, a red spot, a nonhealing ulcer attributed to a sharp cusp or an ill-fitting partial.3 Without a systematic approach to documentation and follow-up, weeks can turn into months. And months, in oncology, matter enormously.4
Erythroplakia, that velvety red lesion that rarely gets enough clinical attention, carries the highest malignant transformation rate of any oral mucosal lesion, yet it is frequently underrecognized. It lacks the dramatic clinical appearance that triggers urgency, because it has the ability to blend in.5 It is usually attributed to trauma, denture irritation, or candidiasis.6
Also by the author: Exploring the emotional roots of oral disease through Biodecoding and Psycho-Neuro-Odontology (PNO)
Oral lichen planus is another chronic lesion where the miss often happens not at diagnosis, but in follow-up. The reticular form is documented once and then forgotten, never tracked for erosive progression, never rebiopsied when the pattern changes. The patient returns year after year, and no one connects the dots.7
And then there are the lesions we dismiss because of the context in which we find them: the leukoplakia in a 35-year-old who “doesn’t fit the profile,” the pigmented lesion in a patient who says it’s always been there, the persistent swelling documented as reactive and never revisited. We pattern-match based on demographic assumptions and miss what the tissue is trying to tell us.8
The common thread? These aren’t always failures of knowledge. They are often failures of systems, of documentation, follow-up, and the habit of trusting our clinical instincts to say: this needs another look.
The emotional weight of “missing something”
The moment a lesion you once dismissed as irritation comes back as carcinoma, your body knows before your mind does. Your breath shortens. Your stomach drops. Your mind replays the scene. Why didn’t I look more carefully? Did I rush? Did I fail them?
This internal dialogue is rarely spoken aloud. The culture of dental hygiene celebrates accuracy and efficiency, but not the emotional reckoning that follows when something is missed. And that silence fosters shame, burnout, and clinical detachment.
What many clinicians don’t realize is that this experience has a name. Second victim syndrome (SVS) refers to the emotional distress, self-doubt, and psychological sequelae that health-care professionals experience following adverse patient outcomes or clinical errors.
First described by Wu in 2000,9 SVS is far more common than most of us admit: global estimates suggest that nearly 50% of health-care providers experience it at least once in their career.10 It can manifest as guilt, anxiety, sleep disturbances, and a profound loss of clinical confidence, and when left unaddressed, it increases the risk of burnout, absenteeism, and even compromised patient care. In dentistry, where the culture still too often equates silence with strength, second victim syndrome thrives in the spaces we don’t talk about.
We must normalize the emotional reality of clinical error. We are not diagnostic machines. Our patients don’t need us to be perfect; they need us to be present, honest, and willing to keep learning.
From time pressure to time presence
Time is one of the most relentless stressors in clinical care. Overbooked days, late patients, incomplete notes … it’s hard to give a thorough oral cancer screening when the clock feels like your enemy.
But here’s the paradox: the fastest dentistry is not always the most efficient. Rushing leads to shortcuts. Shortcuts lead to oversight. Oversight leads to a missed lesion in zone 8 because the exam was moving too fast.
Research confirms what we already feel in our bodies. A 2025 qualitative study published in the British Dental Journal interviewed dental professionals across all team roles and found that time pressure was one of the most universally shared stressors, from clinicians running back-to-back appointments from 9 a.m. to 7 p.m., to support staff who described their days as a “whirlwind from morning to afternoon.”
Critically, the study found that lack of autonomy over how their day was structured was a significant driver of anxiety, while those who had control over their schedule reported greater resilience and fewer clinical errors.11 In other words, time isn’t just a logistical problem; it’s a psychological one. When we lose control of our pace, we lose clinical presence.
Rather than chasing time, we can reclaim presence. Try reframing each patient encounter as a clinical story waiting to be read, not just a procedure to complete. Allow yourself 60 extra seconds on that lesion that doesn’t quite fit. Document it. Photograph it. Give it a follow-up date. These micro-pauses create macro-impact: better clinical catches, stronger patient trust, and more mindful practice.
The hardest empathy: The kind you give yourself
Empathy is often framed as something we give our patients. But in pathology work, where the stakes are high and the gray zones are wide, the most important empathy is often the kind we extend inward.
When you’ve missed something, or fear you did, self-compassion sounds like:
- “I did the best I could with the time, knowledge, and awareness I had at that moment.”
- “This doesn’t define my worth; it reveals where I can grow.”
- “If I wouldn’t shame a colleague for this, why am I shaming myself?”
Self-compassion isn’t an escape from accountability. It’s what makes accountability sustainable. And the science backs this up: a 2025 scoping review published in Academic Medicine found that negative emotions—stress, fear, and uncertainty—are directly associated with increased diagnostic errors and suboptimal clinical decisions. But the same review found that positive emotions and cultivated self-awareness actively support diagnostic accuracy and adaptability in clinical reasoning. In other words, how you feel about your clinical judgment shapes the quality of that judgment itself.
That’s why self-compassion lowers cortisol, improves focus, and prevents the emotional shutdown that turns a caring clinician into someone who stops looking closely because they’re afraid of what they’ll find.12,13
The clinician who keeps showing up
Every diagnosis is an act of clarity. Every misdiagnosis is a call for humility. And every moment of uncertainty is an invitation to slow down and look again.
In oral pathology, we will miss things. The tissue doesn’t always cooperate. The presentation isn’t always classic.14 The patient doesn’t always disclose. And we are working in real time, under real pressure, in real human bodies that don’t read textbooks.
But the clinicians who change outcomes are not the ones who never miss. They are the ones who built systems that catch what was missed … who stayed curious enough to revisit … who kept showing up, even when they feared what they’d find, because they cared more about their patient than about their own comfort.
Let your misses sharpen you, not silence you. Let your empathy protect you, not drain you. Let your resilience root you, and let it root you in the practice of looking closely with both clinical rigor and human compassion.
You were never meant to be perfect. You were meant to grow with every patient.
Editor's note: This article appeared in the April/May 2026 print edition of RDH magazine. Dental hygienists in North America are eligible for a complimentary print subscription. Sign up here.
References
- McCord C, Kiss A, Magalhaes MA, Leong IT, Jorden T, Bradley G. Oral squamous cell carcinoma associated with precursor lesions. Cancer Prev Res (Phila). 2021;14(9):873-884. doi:10.1158/1940-6207.CAPR-21-0047
- Iocca O, Sollecito TP, Alawi F, et al. Potentially malignant disorders of the oral cavity and oral dysplasia: a systematic review and meta-analysis of malignant transformation rate by subtype. Head Neck. 2020;42(3):539-555. doi:10.1002/hed.26006
- Akbulut N, Oztas B, Kursun S, Evirgen S. Delayed diagnosis of oral squamous cell carcinoma: a case series. J Med Case Rep. 2011;5:291. doi:10.1186/1752-1947-5-291
- Singh T, Schenberg M. Delayed diagnosis of oral squamous cell carcinoma following dental treatment. Ann R Coll Surg Engl. 2013;95(5):369-373. doi:10.1308/003588413X13629960045599
- Wadde KR, Gajare PP, Sachdev SS, Singhavi HR. Prevalence and malignant transformation rate of oral erythroplakia worldwide – a systematic review. Ann Maxillofac Surg. 2024;14(1):76-80. doi:10.4103/ams.ams_181_23
- Keinänen A, Uittamo J, Snäll J. Do we recognize oral cancer? Primary professional delay in diagnosis of oral squamous cell carcinoma. Clin Oral Investig. 2024;28(2):131. doi:10.1007/s00784-024-05515-7
- Speight PM, Khurram SA, Kujan O. Oral potentially malignant disorders: risk of progression to malignancy. Oral Surg Oral Med Oral Pathol Oral Radiol. 2018;125(6):612-627. doi:10.1016/j.oooo.2017.12.011
- Vail M, Robinson S, Condon H. Recognition of oral potentially malignant disorders and transformation to oral cancer. JAAPA. 2020;33(11):14-18. doi:10.1097/01.JAA.0000718268.52634.59
- Wu AW. Medical error: the second victim. The doctor who makes the mistake needs help too. BMJ. 2000;320(7237):726-727. doi:10.1136/bmj.320.7237.726
- Ong TSK, Goh CN, Tan EKYE, et al. Second victim syndrome among healthcare professionals: a systematic review of interventions and outcomes. J Healthc Leadersh. 2025;17:225-239. doi:10.2147/JHL.S526565
- Harris M, Eaton K. Exploring dental professionals’ perceptions of resilience to dental environment stress: a qualitative study. Br Dent J. 2025;238(6):395-402. doi:10.1038/s41415-024-7953-z
- Merkebu J, Soh MY, Loncharich M, et al. Emotions and clinical reasoning in medical education and clinical practice: a scoping review. Acad Med. 2025;100(11):e80-e90. doi:10.1097/ACM.0000000000006182
- Neff KD, Knox MC, Long P, Gregory K. Caring for others without losing yourself: an adaptation of the Mindful Self-Compassion Program for Healthcare Communities. J Clin Psychol. 2020;76(9):1543-1562. doi:10.1002/jclp.23007
- Lewis JS Jr. “So you made a mistake” – the path forward through surgical pathology errors by extreme ownership and a focus on the patient. Head Neck Pathol. 2024;18(1):95. doi:10.1007/s12105-024-01706-6
About the Author

Andreina Sucre, MSc, RDH
Andreina Sucre, MSc, RDH, is an international dentist, oral pathology, and oral surgery specialist practicing dental hygiene in Miami, Florida. A passionate advocate for early pathological diagnosis, she empowers colleagues through lectures focused on oral pathologies. Andreina is the founder of The Patho RDH, a published author for RDH magazine, and a selected speaker at RDH Under One Roof 2026. Committed to community outreach, she educates non-native English-speaking children on oral health and actively volunteers in dental initiatives.