Dental hygiene care: Face and neck screening

Authors:
Michele White, DDS
Emelie E. Nelson, BS
John K. McQuitty, MS
Joseph D. Yadin, BS
Gary N. Frey, DDS
Cleverick (C.D.) Johnson, DDS, MS
Kelly C. Nelson, MD
Ben F. Warner, DDS, MD, MS
Athorough inspection of the skin of the face and neck is an essential component of a comprehensive head and neck cancer screening of the dental patient. Any unfamiliar or newly detected lesion can be identified, assessed, and referred as needed for treatment. This guide can help dental professionals become familiar with the appearance of these common skin lesions.
Carefully inspecting the cutaneous and mucosal lips, face, and anterior neck is one way the dental team can display an appreciation for overall health to new or established dental patients. Although skin growths vary in appearance, careful observation offers a unique opportunity for skin cancer detection. Given their frequent encounters with patients, dental hygienists are uniquely positioned to be first-line health-care detectors of skin cancers.
A literature review of common face and neck dermatologic lesions was conducted for this article. Examples and descriptions of frequently encountered skin lesions are included to facilitate recognition by dental professionals.
Lesions can be classified by their color. Going forward, lesions will be classified as pink lesions or brown lesions.


Types of pink lesions
Basal cell carcinoma: Basal cell carcinomas (figures 1-4), the most common form of skin cancer, characteristically present as pink, pearly papules with arborizing blood vessels.1,2 Basal cell carcinomas are prone to bleed spontaneously or with minimal trauma. A common patient narrative is that a pink bump will bleed upon patting their face dry after washing.




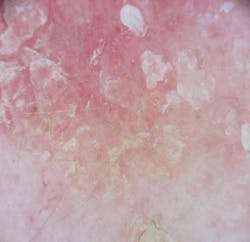
Actinic keratosis: Actinic keratoses (figures 5-7) are premalignant lesions that result from chronic sun damage. In fact, 1%–10% of actinic keratoses may progress to early squamous cell carcinoma. Clinically, actinic keratoses present as rough, scaly pink or flesh-colored patches.3 Actinic cheilitis (sailor’s lip) is a presentation of actinic keratoses on the mucosal surface of the lip.4 The lower lip is more commonly involved than the upper mucosal lip.


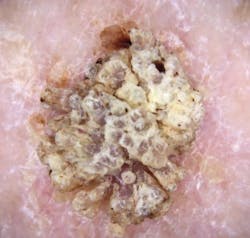
Squamous cell carcinoma: Squamous cell carcinomas (figures 8-12) characteristically present as flesh-colored to pink to red papules, nodules, or plaques with well-defined borders. Central scale or opaque yellow/white keratin and trapped hemorrhage can be present.1 Aggressive squamous cell carcinomas may present as chronic sores or ulcers that extend into the skin.





Types of brown lesions
Seborrheic keratosis: Seborrheic keratoses (figures 13-16) are benign papules or plaques that characteristically have a “stuck on” or “waxy” appearance with well-defined borders.5



Malignant melanoma: Melanomas (figures 17-21) on the face usually present as an asymmetric patch with multiple colors and irregular borders.1 Facial melanoma—unlike normal brown facial growths—is usually a “clinical outlier”; nothing else on the face looks similar.





Discussion
The neck and face are common sites for the development of both benign and malignant skin growths. The risk of skin cancer on the face and neck is higher than on other areas of the body given cumulative sun exposure over time. It is important that dental professionals be able to recognize normal and malignant skin lesions of the face and neck to refer patients for further evaluation. Below are descriptions of the lesions, classified by their color, that dental professionals will most likely encounter.
Pink lesions, classified
Basal cell carcinoma is the most common form of skin cancer, representing approximately 75% of all nonmelanoma skin cancers.6 These lesions appear on sun-exposed areas such as the face, scalp, neck, and ears as pink, pearly (or shiny appearing) flat or raised areas.1 While these lesions grow slowly and rarely metastasize, if left untreated some basal cells may invade into surrounding structures, complicating surgical excision and repair.
Actinic keratoses represent another common, precancerous lesion that often presents as flaky or crusted spots on a background of sun-damaged skin.3 While these spots are not inherently cancerous, if left untreated approximately 1%–10% will progress to become a squamous cell carcinoma.7
Actinic cheilitis, also known as sailor’s lip, appears as confluent actinic keratoses of the lips, most commonly of the exposed mucosal lower lip.4 Actinic cheilitis, like actinic keratosis, is a premalignant condition or precursor to squamous cell carcinoma. Furthermore, squamous cell carcinoma of the lips has a higher risk of metastatic spread (11%) compared to squamous cells arising on the rest of the skin (a 1% metastasis risk). As such, early recognition and treatment of actinic cheilitis is important. This condition is most common in men, the elderly, and patients with fair skin and a history of significant sun exposure.
Squamous cell carcinomas present as pink, red, or flesh-colored nodules or papules, often with scale, crust, erosion, or ulceration.1 Although these lesions do not display a high risk of metastasis, they have the potential for local invasion and can be disfiguring if not treated early. A squamous cell carcinoma should also be suspected with nonhealing sores. Patients who are immunocompromised, have chronic lymphocytic leukemia, or have received a solid organ transplant are at higher risk of developing a squamous cell skin cancer.8
Brown lesions, classified
Seborrheic keratoses represent a common brown lesion likely to be encountered by dental professionals.5 These growths appear as “stuck-on” papules and plaques with well-defined borders, often with a waxy or oily appearance. Seborrheic keratoses are completely benign and tend to appear in adults over the age of 30 with a strong family association. Often, these growths are totally asymptomatic; however, they can become itchy or painful when traumatized or irritated. To evaluate a seborrheic keratosis, a light can be held parallel to the lesion. This will highlight the translucency and texture of the lesion, clues that a lesion is a seborrheic keratosis.
Melanoma is the most worrisome, “can’t miss” brown lesion of which dental professionals should be aware. Most melanomas appear to arise de novo, although about 30% may be associated with a nevus.9 Most melanomas are pigmented; rarely, some may contain little to no pigment and are referred to as amelanotic.
Dental professionals should especially be aware of lentigo maligna melanoma as it most commonly occurs on the face and other sun-exposed areas. Identification of potential lentigo maligna melanomas can be aided by recognizing lesions that are evolving (or changing) and that are clinical outliers (or “ugly ducklings”). Elderly patients may have multiple brown areas on their face, but most benign brown lesions appear as a cohort, with other similar-appearing areas elsewhere on the face. The chances of multiple synchronous facial melanomas are low, thus the presence of other similar-appearing areas elsewhere on the patient’s face is reassuring.

When to refer a lesion for further evaluation
At times, distinguishing among the numerous benign and malignant skin growths with which a patient can present can be challenging. In general, a lesion should be referred to a dermatologist if any of the following criteria are met:
- The lesion is bleeding, ulcerated, or a sore that will not heal.
- The lesion is an “ugly duckling”; i.e., the patient has no other lesion that is similar in appearance to the lesion in question.
- The lesion is evolving or changing in size, shape, or color.
- The lesion is causing great distress to the patient.
Dental professionals are in a strategic position to detect concerning skin lesions of the head, face, and neck as thorough inspection of these regions is routine. As such, it is imperative to become familiar with the most commonly encountered skin lesions and know when to refer a patient to a dermatologist for further evaluation.
Editor's note: This article appeared in the April/May 2024 print edition of RDH magazine. Dental hygienists in North America are eligible for a complimentary print subscription. Sign up here.
References
- Linares MA, Zakaria A, Nizran P. Skin cancer. Prim Care. 2015;42(4):645-659. doi:10.1016/j.pop.2015.07.006
- Weber P, Tschandl P, Sinz C, Kittler H. Dermatoscopy of neoplastic skin lesions: recent advances, updates, and revisions. Curr Treat Options Oncol. 2018;19(11):56. doi:10.1007/s11864-018-0573-6
- Firnhaber JM. Basal cell and cutaneous squamous cell carcinomas: diagnosis and treatment. Am Fam Physician. 2020;102(6):339-346.
- Muse ME, Crane JS. Actinic cheilitis. StatPearls Publishing; 2023. https://www.ncbi.nlm.nih.gov/books/NBK551553/
- Hafner C, Vogt T. Seborrheic keratosis. J Dtsch Dermatol Ges. 2008;6(8):664-677. doi:10.1111/j.1610-0387.2008.06788.x
- Nakayama M, Tabuchi K, Nakamura Y, Hara A. Basal cell carcinoma of the head and neck. J Skin Cancer. 2011;2011:496910. doi:10.1155/2011/496910
- Fuchs A, Marmur E. The kinetics of skin cancer: progression of actinic keratosis to squamous cell carcinoma. Dermatol Surg. 2007;33(9):1099-1101. doi:10.1111/j.1524-4725.2007.33224.x
- Lai M, Pampena R, Cornacchia L, et al. Cutaneous squamous cell carcinoma in patients with chronic lymphocytic leukemia: a systematic review of the literature. Int J Dermatol. 2022;61(5):548-557. doi:10.1111/ijd.15813
- Damsky WE, Bosenberg M. Melanocytic nevi and melanoma: unraveling a complex relationship. Oncogene. 2017;36(42):5771-5792. doi:10.1038/onc.2017.189
Michele White, DDS, is a general dentist and an assistant professor of restorative dentistry at the UTHealth School of Dentistry where she teaches predoctoral dental students in the preclinic simulation laboratory as well as in the dental clinic. She is the course director for the foundational skills for clinic I and II courses that introduce entry-level dental knowledge and skills to first-year dental students. Dr. White provides dental care to patients in the faculty practice at UT Dentists.
About the Author

Michele White, DDS
Michele White, DDS, is a general dentist and an assistant professor of restorative dentistry at the UTHealth School of Dentistry where she teaches predoctoral dental students in the preclinic simulation laboratory as well as in the dental clinic. She is the course director for the foundational skills for clinic I and II courses that introduce entry-level dental knowledge and skills to first-year dental students. Dr. White provides dental care to patients in the faculty practice at UT Dentists.