Case #5
By Joen Iannucci Haring
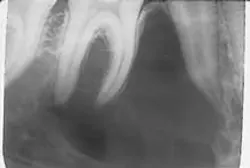
An 18-year-old male visited a dental office for his annual checkup. Radiographic examination revealed a large radiolucency in the right posterior mandible.
History
The patient was unaware of the lesion in the right mandible. He denied any history of pain or sensitivity in the area. When questioned about trauma to the area, the patient stated that he had previously sustained minor blows to the lower jaw while boxing. At the time of the dental appointment, the patient appeared to be in a general good state of health with no significant medical history. His dental history included routine checkups.
Examinations
The patient's vital signs were all found to be within normal limits. Extraoral examination of the head and neck region revealed no enlarged or palpable lymph nodes. Intraoral examination revealed no bony or soft tissue abnormalities present.

Radiographic examination revealed a solitary well-defined radiolucency in the right mandible (see film). The radiolucency appeared large with inter-radicular scalloping and well-defined borders. The lesion appeared to extend around and between the roots of the adjacent teeth. The roots of the teeth surrounded by the lesion appeared to exhibit an intact lamina dura and periodontal ligament space. The teeth adjacent to the radiolucency tested vital.
Clinical diagnosis
Based on the clinical and radiographic information presented, which one of the following is the most likely diagnosis?
o odontogenic keratocyst
o primordial cyst
o simple bone cyst
o ameloblastoma
o central giant cell granuloma
Diagnosis
• simple bone cyst
Discussion
The simple bone cyst (also known as the traumatic bone cyst) is a lesion that affects the long bones of the body as well as the mandible. The simple bone cyst is not a true cyst. A true cyst exhibits an epithelial lining; this lesion does not. The cause of the simple bone cyst is uncertain, although as the name traumatic suggests, trauma is suspected. It is believed that the simple bone cyst is seen as the sequelae of trauma. Approximately one half of the patients with this lesion report a history of trauma to the affected area. Investigators believe that, after trauma to the area, a hematoma forms within the bone. Then, instead of organizing, it breaks down, leaving an empty cavity.
Clinical features
The simple bone cyst is most often seen in young people, ages 10 to 20. Males are affected more frequently than females. When the jaws are involved, the simple bone cyst only affects the mandible, and the premolar and molar areas are most often involved. The simple bone cyst is typically asymptomatic. When symptoms are present, 20 percent of cases include expansion of the bone while less than 10 percent of cases include pain. The lesion is not seen in association with pulpal problems and the teeth that approximate the lesion pulp-test vital.
Radiographic features
On a radiograph, the simple bone cyst appears as a solitary unilocular radiolucency with well-defined margins that exhibit a characteristic inter-radicular scalloping. The term scalloping refers to the borders of the lesion that curve and extend between the surfaces of adjacent tooth roots.
In a small number of cases, the simple bone cyst may appear as a multilocular radiolucency. Although most simple bone cysts measure less than 3 centimeters in diameter, the lesion size is variable and can range from 1 to 10 centimeters in diameter. The lamina dura and periodontal ligament space of the adjacent teeth appear intact. The simple bone cyst rarely displaces teeth, destroys roots, or perforates cortical bone.
The simple bone cyst cannot be diagnosed from a radiograph alone. Other lesions that may resemble a simple bone cyst on a radiograph include the odontogenic keratocyst, ameloblastoma, or central giant cell granuloma.
Diagnosis and treatment
In order to make a definitive diagnosis, the simple bone cyst must be surgically explored. When the area of affected bone is surgically opened and examined, a straw-colored fluid or an empty cavity of bone is identified.
The recommended treatment for the simple bone cyst is curettage. Curettage of the bony walls stimulates bleeding and the organization of a blood clot followed by fibroblastic activity and osseous repair. The lesion fills with bone over a period of six to 12 months.
Periodic post-surgical radiographs may be used to evaluate the resolution of the lesion. Eventually, the lesion exhibits a normal bony appearance on follow-up radiographs. Recurrence or persistence of the simple bone cyst is unusual.
Joen Iannucci Haring, DDS, MS, is a professor of clinical dentistry, Section of Primary Care, The Ohio State University College of Dentistry.