Periapical cemento-osseous dysplasia

Your patient today is Mei-Yin, a 55-year-old Asian female who is being seen for a routine prophylaxis. She needs radiographs, and, after evaluating the images, you are concerned about the radiolucent apical area on No. 24. She is currently taking medication for acid reflux and occasionally uses ibuprofen for joint discomfort. She also takes Zyrtec (10mg. qd) for seasonal allergies.
Mei-Yin states that she does not have any pain related to her teeth. She has some periodontal bone loss and calculus, but is otherwise very healthy. Some mobility of the mandibular teeth is noted, and no lymphadenopathy is evident. She does not remember any previous trauma to this area of her mouth. You explain to her that the concern is the area in the apical region of her mandibular tooth and you show her the area of concern on the radiograph. Palpation of the area is crucial, as well as a thorough oral exam and cancer screening.
Radiolucent areas usually indicate that there is an infection present or that there may be a cyst or possibly a
Cemento-osseous dysplasia (COD) is an asymptomatic benign condition with an unknown etiology or pathogenesis.
- There are three types of cemento-osseous dysplasia that have been documented:
- Periapical cemento-osseous dysplasia (occurring in the anterior mandible region).
- Focal cemento-osseous dysplasia (occurring in areas other than the apical region and a propensity for the posterior mandible region).
- Florid cemento-osseous dysplasia (may be confused with a simple bone cyst). This type must be differentiated from Paget’s disease, chronic diffuse osteomyelitis, and Gardner’s syndrome.
All three types are asymptomatic, and the patient is usually unaware that any changes have occurred until a radiographic examination causes the clinician to become concerned. However, depending upon the advancement of the lesion, clinical signs may be present as well. Although the etiology is not known, it is believed to be a reactive process that is not contagious and it is considered benign. However, other more serious disease states need to be ruled out. The COD occurs primarily in those over age 40, usually middle age, predominately women (Melrose, 1975), and they have been reported in blacks, Asians, as well as Caucasians. The entity was previously referred to in the literature as the cementoma.
With cases of cemento-osseous dysplasia, confusion can occur when the clinician believes that the tooth may need a root canal or extraction based on the radiographic appearance. Three variations may occur in the clinical appearance (Komabayashi and Zhu, 2011) such as:
- Early stage (radiolucency without radiopacity inclusion)
- Mixed stage (radiolucency with radiopacity inclusion)
- Mature stage (radiopacity). This stage is more radiopaque, but, as you can imagine, the degree of both radiolucent and radiopaque appearances may vary greatly.
Generally, there is suspicion of a diseased state whether a mixed radiolucent area or opaque lesion is present. A diagnostic investigation would include testing for percussion, palpation, cold testing (ice), and an electric pulp test. Periapical cemento-ossifying dysplasia would present with a vital pulp.
Differential diagnosis of such lesions would include odontoma, cemento-ossifying fibroma, hypercementosis, cementoblastoma, and ossifying fibroma.
Clinical appearances, health implications, ethnicity, and age would be factors that the practitioner would take into consideration in a diagnosis. The key factor involving the periapical cemento-osseous dysplasia is pulp testing. The tooth will test vital.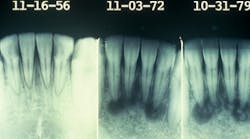
A periapical inflammatory lesion may be diagnosed if pulp testing is not performed and a diagnostic workup is not performed as part of the treatment plan. The patient may be referred for endodontic treatment (root canal) when it is not necessary.
Often, the periapical cemento-osseous dysplasia can be followed when the patient is seen periodically over a long period of time. The second image presented here occurred over a 23-year period with observation (see Figure 2).
Remember to keep asking good questions and always listen to your patients.
References
Alsufyani NA, Lam EWN. Osseous (cemento-osseous) dysplasia of the jaws: Clinical and Radiographic Analysis. J Can Dent Assoc 2011; 77:b70.
DeLong L, Burkhart NW. General and Oral Pathology for the Dental Hygienist. Lippincott, Williams & Wilkins. Baltimore. 2008.
Kim JH, Song BC, Kim SH, Park YS. Clinical, radiographic and histological findings of florid cemento-osseous dysplasia: a case report. Imaging Sci Dent.2011; 41: 139-142.
Kombayashi T, Zhu Q. Cemento-osseous dysplasia in an elderly Asian male: a case report. J Oral Science 2011; 53(1):117-120.
Melrose RJ, Abrams AM, Mills BG. Florid osseous dysplasia. A clinical-pathological study of thirty-four cases. Oral Surg Oral Med Oral Pathol 1976;41(1): 62-82.

Nancy W. Burkhart, BSDH, EdD, is an adjunct associate professor in the department of periodontics, Baylor College of Dentistry and the Texas A & M Health Science Center, Dallas. Dr. Burkhart is founder and cohost of the International Oral Lichen Planus Support Group (http://bcdwp.web.tamhsc.edu/iolpdallas/) and coauthor of General and Oral Pathology for the Dental Hygienist. She was a 2006 Crest/ ADHA award winner. Her website for seminars is www.nancywburkhart. com.
Past RDH Issues